Resumo
Definição
História e exame físico
Principais fatores diagnósticos
- presença de fatores de risco
- infecções recorrentes e incomumente graves
- diarreia crônica
- retardo do crescimento pôndero-estatural
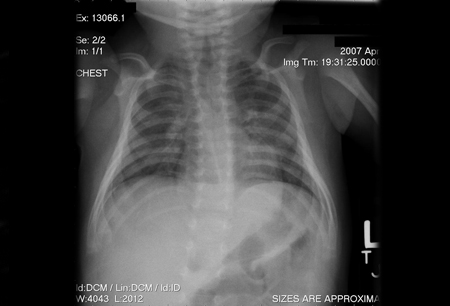
- ausência do tecido linfoide
Outros fatores diagnósticos
- erupção cutânea
- úlceras orais ou genitais
- microcefalia
- anormalidades esqueléticas
- cegueira
- distonia
- sensibilidade à radiação
Fatores de risco
- História familiar de IDCG
- História familiar de morte infantil
- Índios norte-americanos falantes de atabascano
- Consanguinidade
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- Hemograma completo
- citometria de fluxo
- radiografia torácica
- teste quantitativo de imunoglobulinas (IgG, IgM e IgA)
Investigações a serem consideradas
- ultrassonografia do tórax
- TC do tórax
- ressonância nuclear magnética (RNM) do tórax
- fundoscopia
- testes enzimáticos
- ácido úrico sérico
- estudos de proliferação de células T
- testagem da viremia baseada em reação em cadeia da polimerase
- sensibilidade à radiação das culturas de fibroblastos
- teste genético
Algoritmo de tratamento
Colaboradores
Autores
Javier Chinen, MD, PhD
Professor
Pediatrics, Allergy, and Immunology
Baylor College of Medicine
Texas Children’s Hospital
Houston
TX
Declarações
JC declares that he has no competing interests.
Agradecimentos
Dr Chinen would like to gratefully acknowledge Dr John M. Cunningham, Dr James L. LaBelle, Dr John Routes, Dr James Verbsky, Dr Nicole Chase, and Dr Ebrahim Shakir, the previous contributors to this topic.
Declarações
JLL, JR, JV, and NC are authors of references cited in this topic. JMC and ES declare that they have no competing interests.
Revisores
Elizabeth Secord, MD
Professor of Pediatrics
Division of Immunology
Wayne State University School of Medicine
Detroit
MI
Declarações
ES declares that she has no competing interests.
Waseem Qasim, BMedSci (Hons), MBBS, MRCP (UK), MRCPCH, PhD
Senior Lecturer
Institute of Child Health
Consultant in Paediatric Immunology & Bone Marrow Transplantation
Great Ormond Street Hospital
London
UK
Declarações
WQ declares that he has no competing interests.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
Bousfiha A, Moundir A, Tangye SG, et al. The 2022 update of IUIS phenotypical classification for human inborn errors of immunity. J Clin Immunol. 2022 Oct 6 [Epub ahead of print]. Resumo
Tangye SG, Al-Herz W, Bousfiha A, et al. Human inborn errors of immunity: 2022 update on the classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol. 2022 Jun 24;1-35 [Epub ahead of print].Texto completo Resumo
Bonilla FA, Khan DA, Ballas ZK, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. 2015 Nov;136(5):1186-205.e1-78.Texto completo Resumo
Buckley RH. Molecular defects in human severe combined immunodeficiency and approaches to immune reconstitution. Ann Rev Immunol. 2004:22:625-55. Resumo
Heimall J, Buckley RH, Puck J, et al. Recommendations for screening and management of late effects in patients with severe combined immunodeficiency after allogenic hematopoietic cell transplantation: a consensus statement from the second pediatric blood and marrow transplant consortium international conference on late effects after pediatric HCT. Biol Blood Marrow Transplant. 2017 Aug;23(8):1229-40.Texto completo Resumo
Candotti F, de Villartay JP, Moshous D, et al. Severe combined immune deficiency. In: Sullivan KE, Stiehm ER, eds. Stiehm’s immune deficiencies: inborn errors in immunity. 2nd ed. Cambridge, MA: Academic Press, 2020:153-205.
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível aqui.
O uso deste conteúdo está sujeito ao nosso aviso legal