Investigations
1st investigations to order
stool microscopy
Test
Not as sensitive or specific as other tests but still used clinically to confirm amoebic intestinal infection.[1][2][3][4][5]
Stool microscopy relies on observation of cysts and trophozoites in faeces, colonic scrapings, aspirates and tissue samples.[26] It is not specific for the diagnosis of amoebiasis, as Entamoeba histolytica cysts and trophozoites are indistinguishable from those of Entamoeba dispar, Entamoeba moshkovskii, and Entamoeba bangladeshi.[7][17] While it lacks specificity, stool microscopy has the advantage of being readily available and may demonstrate other infectious causes. The presence of erythrophagocytic trophozoites is highly suggestive of E histolytica infection.
UK guidelines recommend that stool samples which are positive on microscopy for Entamoeba spp. should be sent for confirmatory PCR testing.[26]
Result
identification of Entamoeba in stool
PCR or qPCR of stool or liver abscess pus for Entamoeba histolytica DNA
Test
Where available, PCR is now the method of choice for diagnosis of E histolytica.[7][26] However, cost is a barrier to its use as a routine test in many endemic areas, meaning that laboratory diagnosis in many countries still relies on antigen-detection or microscopy for ova and parasites. PCR and real-time quantitative PCR (qPCR) testing of stool is highly sensitive and specific for the detection of E histolytica.[27] Real-time qPCR is more sensitive than traditional PCR.[27] Stool samples which are positive on microscopy for E histolytica/dispar should be sent for confirmatory PCR testing.[26] Liver abscesses should be aspirated to determine aetiology. The pus should be analysed by PCR or qPCR to identify whether the causal infection is amoebic and cultured to determine whether it is pyogenic.[1][2]
Result
amplification of amoebic DNA
stool antigen detection
Test
Antigen testing on stool samples is an alternative to PCR. Antigen tests have been well studied and have several advantages, including their technical simplicity, relative low cost and rapid turnaround.[26] Only the Cellabs Entamoeba CELISA Path, the TechLab Entamoeba histolytica II, or the TechLab Histological Quik Chek tests specifically identify E histolytica; other antigen detection tests detect the E histolytica-Entamoeba dispar-Entamoeba moshkovskii species complex.[28]
Result
positive for parasite antigen
serum antibody test
Test
In patients with suspected amoebic disease, especially possible liver abscess without concurrent intestinal infection (where there are unlikely to be detectable parasites in stool), serum antibody testing for Entamoeba histolytica can be a useful diagnostic adjunct.[2][7][10][28] Tests for antibodies are approximately 90% sensitive for amoebic liver abscess and 70% sensitive for amoebic colitis.[2] A major problem with serological tests however, is that the patient continues to test positive for years after an episode of amoebiasis; as a result, a substantial number (10% to 35%) of residents of developing countries have antibodies to amoebae. Therefore, negative serology is helpful for exclusion of disease, but positive serology cannot distinguish between acute and previous infection.[2][7]
Result
positive for antiamoebic antibodies
Investigations to consider
colonoscopy
Test
May be helpful if clinical suspicion is high and antigen detection tests are negative.[2] Biopsy specimens should be taken from the edge of an ulcer. Histology may show trophozoites, but the sensitivity of histopathological diagnosis using biopsy samples obtained by colonoscopy is low (45.5%).[29] Endocytoscopy may allow for real-time visualisation of amoebae in the colonic mucosa of patients with colitis.[30][Figure caption and citation for the preceding image starts]: Amoebic ulcerations of the colon: colonic ulcers averaging 1 mm to 2 mm in diameter on gross pathologyReproduced from New England Journal of Medicine (2003); used with permission [Citation ends].
Result
granular, friable, and diffusely ulcerated mucosa
liver ultrasound
CXR
Test
Performed if clinical findings suggestive of effusion and presence of liver abscess. [Figure caption and citation for the preceding image starts]: Posterior-anterior and lateral CXR of a patient with amoebic liver abscess: CXR findings include elevated right hemidiaphragm and evidence of atelectasisReproduced from New England Journal of Medicine (2003); used with permission [Citation ends].
Result
right hemidiaphragm elevation or right-sided pleural effusion
CT liver/chest/head
Test
Unable to distinguish from a pyogenic abscess.[2][Figure caption and citation for the preceding image starts]: Entamoeba histolytica brain abscessReproduced from Transactions of the Royal Society of Tropical Medicine and Hygiene (2007); used with permission [Citation ends].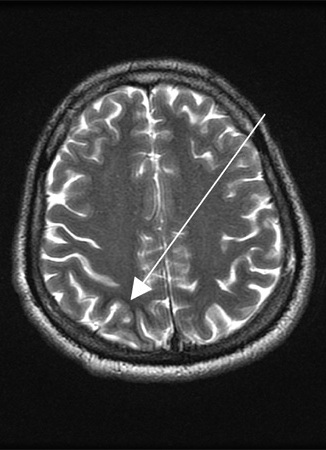
Result
rounded, well-defined, low-attenuation lesion; wall commonly enhances with contrast; pleural effusion
MRI brain
Test
Required if neurological symptoms.
Result
space-occupying lesion(s)
Use of this content is subject to our disclaimer