Confirmatory laboratory tests should be performed before starting therapy for those in whom amoebiasis is suspected. Diagnostic tools include stool antigen detection, stool (or abscess aspirate in the case of extra-intestinal disease) polymerase chain reaction (PCR) testing, stool microscopy, serology, and colonoscopy with histologic examination.
Clinical evaluation
Amoebiasis should be considered in any individual who presents with diarrhoea or liver abscess and who has travelled or lived in an endemic area in the previous 12 months. Other populations at risk of infection are institutionalised individuals (particularly those with intellectual disability), men who have sex with men, and commercial sex workers and their sexual contacts.[14]Nagata N, Shimbo T, Akiyama J, et al. Risk factors for intestinal invasive amebiasis in Japan, 2003-2009. Emerg Infect Dis. 2012 May;18(5):717-24.
https://wwwnc.cdc.gov/eid/article/18/5/11-1275_article
http://www.ncbi.nlm.nih.gov/pubmed/22515839?tool=bestpractice.com
Presentation is subacute in many cases; most patients have a gradual illness onset days or weeks after infection.[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
[10]Centers for Disease Control and Prevention. CDC Yellow Book 2026: health information for international travel. Section 5: travel-associated infections & diseases - travelers’ diarrhea. Apr 2025 [internet publication].
https://www.cdc.gov/yellow-book/hcp/preparing-international-travelers/travelers-diarrhea.html
Key symptoms of infection are diarrhoea that has lasted for several days or longer, and abdominal pain. Entamoeba histolytica diarrhoea may be watery or bloody, and be clinically-indistinguishable from diarrhoea caused by inflammatory bowel disease or a variety of other enteropathogens.[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
Weight loss is reported by about 50% of patients.[1]Haque R, Huston CD, Hughes M, et al. Amebiasis. New Engl J Med. 2003;348:1565-73.
http://www.ncbi.nlm.nih.gov/pubmed/12700377?tool=bestpractice.com
[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
Right upper quadrant (RUQ) abdominal pain in a man aged 20 to 40 years, with or without coincident diarrhoea, could indicate an amoebic liver abscess.[1]Haque R, Huston CD, Hughes M, et al. Amebiasis. New Engl J Med. 2003;348:1565-73.
http://www.ncbi.nlm.nih.gov/pubmed/12700377?tool=bestpractice.com
[2]Petri WA Jr, Singh U. Diagnosis and management of amebiasis. Clin Infect Dis. 1999;29:1117-25.
http://www.ncbi.nlm.nih.gov/pubmed/10524950?tool=bestpractice.com
[3]Solaymani-Mohammadi S, Lam M, Zunt JR. Entamoeba histolytica encephalitis diagnosed by polymerase chain reaction of cerebrospinal fluid. Trans R Soc Trop Med Hyg. 2007;101:311-13.
http://www.ncbi.nlm.nih.gov/pubmed/16930651?tool=bestpractice.com
[4]Watanabe K. Amebiasis. In: Rakel RE, ed. Conn's current therapy 2019. New York, NY: W.B. Saunders; 2019.[5]Stanley SL Jr. Amoebiasis. Lancet. 2003;361:1025-34.
http://www.ncbi.nlm.nih.gov/pubmed/12660071?tool=bestpractice.com
[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
However, prolonged fever can be the only symptom of liver abscess, making early diagnosis challenging. Patients may report altered mental status if brain abscess is present. Amoebic acute appendicitis is a possible but rare manifestation of amoebiasis; amoebic appendicitis is more likely to be complicated than non-amoebic appendicitis.[9]Otan E, Akbulut S, Kayaalp C. Amebic acute appendicitis: systematic review of 174 cases. World J Surg. 2013 Sep;37(9):2061-73.
https://www.doi.org/10.1007/s00268-013-2079-5
http://www.ncbi.nlm.nih.gov/pubmed/23665815?tool=bestpractice.com
Physical examination
Fever is rare with intestinal infection but common with extraintestinal infection (such as liver and brain abscess).[1]Haque R, Huston CD, Hughes M, et al. Amebiasis. New Engl J Med. 2003;348:1565-73.
http://www.ncbi.nlm.nih.gov/pubmed/12700377?tool=bestpractice.com
[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
With hepatic infection, jaundice, RUQ tenderness, and hepatomegaly may also be present. Liver abscesses may extend into the pleural or pericardial cavities (rare), resulting in signs of a pleural or pericardial effusion. Splenic abscess is a rare manifestation of amoebiasis. Neurological abnormalities, such as limb weakness, may be present in patients with a brain abscess.
Laboratory evaluation
Of the available diagnostic tests, antigen testing and PCR can differentiate between E histolytica and the non-pathogenic Entamoeba dispar.[17]Centers for Disease Control and Prevention. CDC Yellow Book 2026: health information for international travel. Section 5: travel-associated infections & diseases - post-travel diarrhea. Apr 2025 [internet publication].
https://www.cdc.gov/yellow-book/hcp/post-travel-evaluation/post-travel-diarrhea.html
PCR has the highest sensitivity and is the method of choice for diagnosis though is a barrier to its use as a routine test in many endemic areas. Laboratory diagnosis of intestinal amoebiasis in many countries still relies on antigen-detection or ova and parasite microscopy.[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
[25]Saidin S, Othman N, Noordin R. Update on laboratory diagnosis of amoebiasis. Eur J Clin Microbiol Infect Dis. 2019 Jan;38(1):15-38.
https://link.springer.com/article/10.1007/s10096-018-3379-3
http://www.ncbi.nlm.nih.gov/pubmed/30255429?tool=bestpractice.com
Microscopy
Stool microscopy relies on observation of cysts and trophozoites in faeces, colonic scrapings, aspirates and tissue samples.[26]Public Health England. Interim public health operational guidelines for amoebiasis (Entamoeba histolytica). Oct 2017 [internet publication].
https://www.gov.uk/government/publications/amoebiasis-public-health-operational-guidelines
It is not specific for the diagnosis of amoebiasis, as E histolytica cysts and trophozoites are indistinguishable from those of E dispar, Entamoeba moshkovskii, and Entamoeba bangladeshi.[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
[17]Centers for Disease Control and Prevention. CDC Yellow Book 2026: health information for international travel. Section 5: travel-associated infections & diseases - post-travel diarrhea. Apr 2025 [internet publication].
https://www.cdc.gov/yellow-book/hcp/post-travel-evaluation/post-travel-diarrhea.html
Historically, E dispar and E moshkovskii have been considered non-pathogenic, but evidence is mounting that E moshkovskii can cause illness.[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
E bangladeshi has only recently been identified, so its pathogenic potential is not well understood. While it lacks specificity, stool microscopy for ova, cysts, and parasites has the advantage of being readily available and may demonstrate other infectious causes. The presence of erythrophagocytic trophozoites is highly suggestive of E histolytica infection. UK guidelines recommend that stool samples which are positive on microscopy for Entamoeba spp. should be sent for confirmatory PCR testing.[26]Public Health England. Interim public health operational guidelines for amoebiasis (Entamoeba histolytica). Oct 2017 [internet publication].
https://www.gov.uk/government/publications/amoebiasis-public-health-operational-guidelines
PCR
Where available, PCR is now the method of choice for diagnosis of E histolytica.[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
[26]Public Health England. Interim public health operational guidelines for amoebiasis (Entamoeba histolytica). Oct 2017 [internet publication].
https://www.gov.uk/government/publications/amoebiasis-public-health-operational-guidelines
PCR and real-time quantitative PCR (qPCR) testing of stool is highly sensitive and specific for the detection of E histolytica.[27]Roy S, Kabir M, Mondal D, et al. Real-time PCR assay for the diagnosis of Entamoeba histolytica Infection. J Clin Microbiol. 2005;43:2168-72.
http://www.ncbi.nlm.nih.gov/pubmed/15872237?tool=bestpractice.com
Real-time qPCR is more sensitive than traditional PCR.[27]Roy S, Kabir M, Mondal D, et al. Real-time PCR assay for the diagnosis of Entamoeba histolytica Infection. J Clin Microbiol. 2005;43:2168-72.
http://www.ncbi.nlm.nih.gov/pubmed/15872237?tool=bestpractice.com
Stool samples which are positive on microscopy for E histolytica/dispar should be sent for confirmatory PCR testing.[26]Public Health England. Interim public health operational guidelines for amoebiasis (Entamoeba histolytica). Oct 2017 [internet publication].
https://www.gov.uk/government/publications/amoebiasis-public-health-operational-guidelines
Liver abscesses should be aspirated to determine aetiology. The pus should be analysed by PCR or qPCR to identify whether the causal infection is amoebic and cultured to determine whether it is pyogenic.[1]Haque R, Huston CD, Hughes M, et al. Amebiasis. New Engl J Med. 2003;348:1565-73.
http://www.ncbi.nlm.nih.gov/pubmed/12700377?tool=bestpractice.com
[2]Petri WA Jr, Singh U. Diagnosis and management of amebiasis. Clin Infect Dis. 1999;29:1117-25.
http://www.ncbi.nlm.nih.gov/pubmed/10524950?tool=bestpractice.com
Antigen testing
Antigen testing on stool samples is an alternative to PCR. Antigen tests have been well studied and have several advantages, including their technical simplicity, relative low cost and rapid turnaround.[26]Public Health England. Interim public health operational guidelines for amoebiasis (Entamoeba histolytica). Oct 2017 [internet publication].
https://www.gov.uk/government/publications/amoebiasis-public-health-operational-guidelines
Available testing kits include the TechLab E histolytica II (ELISA), the TechLab E. HISTOLYTICA QUIK CHEK, or The Cellabs Entamoeba CELISA Path. These are highly specific for E histolytica; other detection kits detect the E histolytica-E dispar-E moshkovskii species complex.[28]Haque R, Mollah NU, Ali IKM, et al. Diagnosis of amebic liver abscess and intestinal infection with the TechLab Entamoeba histolytica II antigen detection and antibody tests. J Clin Microbiol. 2000;38:3235-39.
http://jcm.asm.org/cgi/content/full/38/9/3235?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&searchid=1&FIRSTINDEX=0&volume=38&firstpage=3235&resourcetype=HWCIT
Serum antibody testing
In patients with suspected amoebic disease, especially possible liver abscess without concurrent intestinal infection (where there are unlikely to be detectable parasites in the stool), serum antibody testing for E histolytica can be a useful diagnostic adjunct.[2]Petri WA Jr, Singh U. Diagnosis and management of amebiasis. Clin Infect Dis. 1999;29:1117-25.
http://www.ncbi.nlm.nih.gov/pubmed/10524950?tool=bestpractice.com
[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
[10]Centers for Disease Control and Prevention. CDC Yellow Book 2026: health information for international travel. Section 5: travel-associated infections & diseases - travelers’ diarrhea. Apr 2025 [internet publication].
https://www.cdc.gov/yellow-book/hcp/preparing-international-travelers/travelers-diarrhea.html
[28]Haque R, Mollah NU, Ali IKM, et al. Diagnosis of amebic liver abscess and intestinal infection with the TechLab Entamoeba histolytica II antigen detection and antibody tests. J Clin Microbiol. 2000;38:3235-39.
http://jcm.asm.org/cgi/content/full/38/9/3235?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&searchid=1&FIRSTINDEX=0&volume=38&firstpage=3235&resourcetype=HWCIT
Tests for antibodies are approximately 90% sensitive for amoebic liver abscess and 70% sensitive for amoebic colitis.[2]Petri WA Jr, Singh U. Diagnosis and management of amebiasis. Clin Infect Dis. 1999;29:1117-25.
http://www.ncbi.nlm.nih.gov/pubmed/10524950?tool=bestpractice.com
A major problem with serological tests however, is that the patient continues to test positive for years after an episode of amoebiasis; as a result, a substantial number (10% to 35%) of residents of developing countries have antibodies to amoebae. Therefore, negative serology is helpful for exclusion of disease, but positive serology cannot distinguish between acute and previous infection.[2]Petri WA Jr, Singh U. Diagnosis and management of amebiasis. Clin Infect Dis. 1999;29:1117-25.
http://www.ncbi.nlm.nih.gov/pubmed/10524950?tool=bestpractice.com
[7]Shirley DT, Farr L, Watanabe K, et al. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018 Jul;5(7):ofy161.
https://academic.oup.com/ofid/article/5/7/ofy161/5049601
http://www.ncbi.nlm.nih.gov/pubmed/30046644?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Cyst of Entamoeba histolytica: unstained (A), and iodine stained (B) after formalin-ether concentration of stool sample.Original photos from National Center for Global Health and Medicine, Tokyo, Japan. [Citation ends].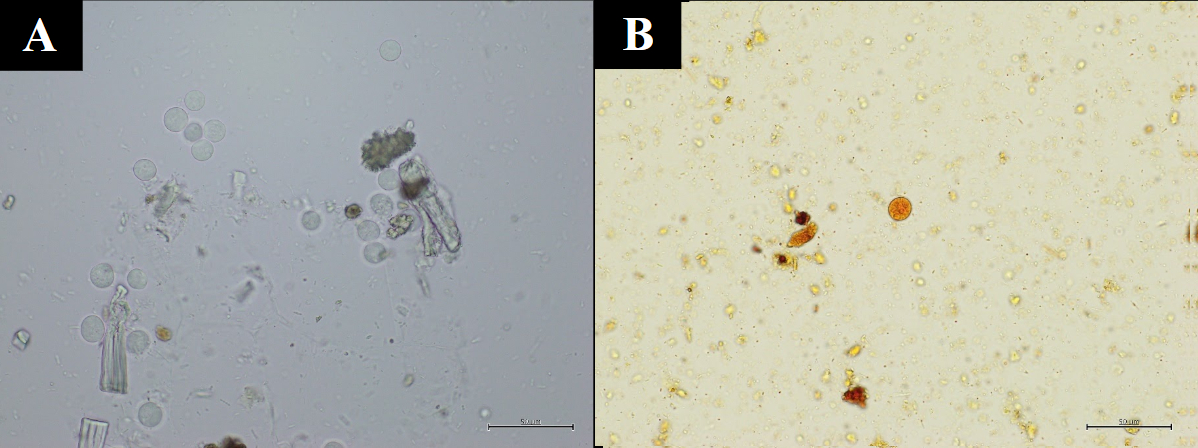
[Figure caption and citation for the preceding image starts]: Cyst of Entamoeba histolytica: iodine stain of stool sampleReproduced from Current Concepts (2003); used with permission [Citation ends].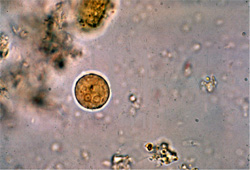 [Figure caption and citation for the preceding image starts]: Trophozoites of Entamoeba histolytica: trichrome stain of stool sampleReproduced from Clinical Infectious Diseases (1999); used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Trophozoites of Entamoeba histolytica: trichrome stain of stool sampleReproduced from Clinical Infectious Diseases (1999); used with permission [Citation ends].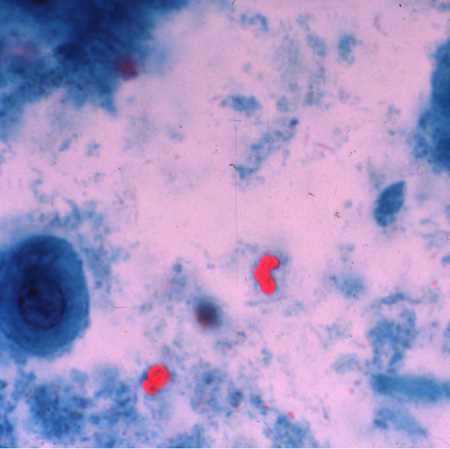 [Figure caption and citation for the preceding image starts]: Trophozoite of Entamoeba histolytica with pseudopod (red arrow): direct unstained stool sample.Original photo from National Center for Global Health and Medicine, Tokyo, Japan. [Citation ends].
[Figure caption and citation for the preceding image starts]: Trophozoite of Entamoeba histolytica with pseudopod (red arrow): direct unstained stool sample.Original photo from National Center for Global Health and Medicine, Tokyo, Japan. [Citation ends].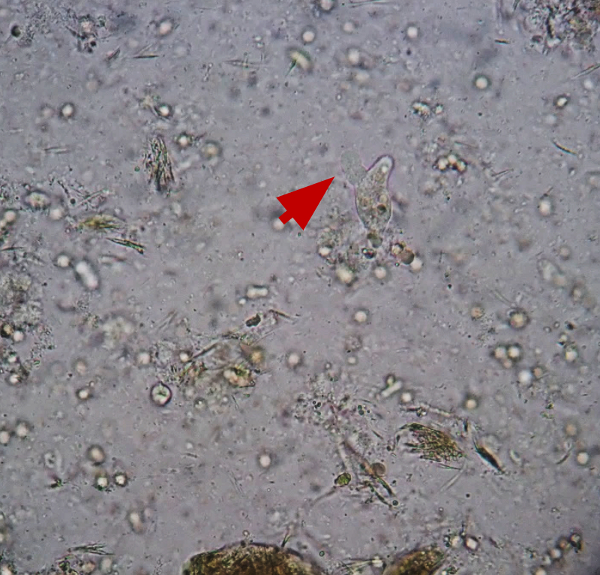
Colonoscopy
May be helpful if clinical suspicion is high and antigen detection tests are negative.[2]Petri WA Jr, Singh U. Diagnosis and management of amebiasis. Clin Infect Dis. 1999;29:1117-25.
http://www.ncbi.nlm.nih.gov/pubmed/10524950?tool=bestpractice.com
Biopsy specimens should be taken from the edge of an ulcer. Histology may show trophozoites, but the sensitivity of histopathological diagnosis using biopsy samples obtained by colonoscopy is low (45.5%).[29]Yanagawa Y, Nagata N, Yagita K, et al. Clinical features and gut microbiome of asymptomatic entamoeba histolytica infection. Clin Infect Dis. 2021 Nov 2;73(9):e3163-71.
https://www.doi.org/10.1093/cid/ciaa820
http://www.ncbi.nlm.nih.gov/pubmed/32564059?tool=bestpractice.com
Endocytoscopy may allow for real-time visualisation of amoebae in the colonic mucosa of patients with colitis.[30]Hosoe N, Kobayashi T, Kanai T, et al. In vivo visualization of trophozoites in patients with amoebic colitis by using a newly developed endocytoscope. Gastrointest Endosc. 2010;72:643-6.
http://www.ncbi.nlm.nih.gov/pubmed/20579647?tool=bestpractice.com
Amoebiasis is occasionally diagnosed during detailed examination to investigate chronic diarrhoea and positive results on faecal occult blood testing.[31]Spinzi G, Pugliese D, Filippi E. An Unexpected Cause of Chronic Diarrhea. Gastroenterology. 2016 Jan;150(1):e5-6.
https://www.doi.org/10.1053/j.gastro.2015.05.054
http://www.ncbi.nlm.nih.gov/pubmed/26627328?tool=bestpractice.com
[32]Okamoto M, Kawabe T, Ohata K, et al. Amebic colitis in asymptomatic subjects with positive fecal occult blood test results: clinical features different from symptomatic cases. Am J Trop Med Hyg. 2005 Nov;73(5):934-5.
http://www.ncbi.nlm.nih.gov/pubmed/16282306?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Amoebic ulcerations of the colon: colonic ulcers averaging 1 mm to 2 mm in diameter on gross pathologyReproduced from New England Journal of Medicine (2003); used with permission [Citation ends].
Imaging
If liver involvement is suspected, a liver ultrasound should initially be performed. CXR and chest/abdominal CT are indicated if an effusion due to abscess extension is suggested by clinical findings.
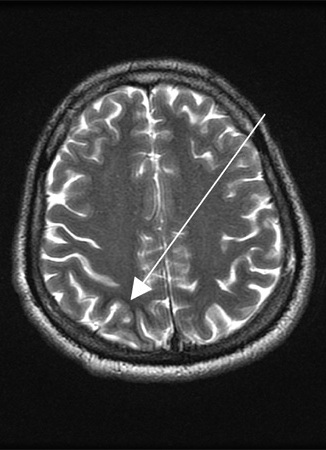
Patients with neurological symptoms should have a CT or MRI of the brain.[1]Haque R, Huston CD, Hughes M, et al. Amebiasis. New Engl J Med. 2003;348:1565-73.
http://www.ncbi.nlm.nih.gov/pubmed/12700377?tool=bestpractice.com
[5]Stanley SL Jr. Amoebiasis. Lancet. 2003;361:1025-34.
http://www.ncbi.nlm.nih.gov/pubmed/12660071?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: Posterior-anterior and lateral CXR of a patient with amoebic liver abscess: CXR findings include elevated right hemidiaphragm and evidence of atelectasisReproduced from New England Journal of Medicine (2003); used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Entamoeba histolytica brain abscessReproduced from Transactions of the Royal Society of Tropical Medicine and Hygiene (2007); used with permission [Citation ends].