Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
urgent surgical repair
The treatment of unstable SCFE is similar to that of stable SCFE. However, there are differences regarding timing of the surgery, decompression of hip joint, incidental reduction of the SCFE, and stabilisation method with 1 or 2 screws.[Figure caption and citation for the preceding image starts]: Unstable SCFE of the right hip fixed with 2 screws. Left hip prophylactic fixation with a single screw. Antero-posterior post-operative x-rayImage courtesy of John M. Flynn, MD [Citation ends]. [Figure caption and citation for the preceding image starts]: Unstable SCFE of the right hip fixed with 2 screws. Left hip prophylactic fixation with a single screw. Frog-leg lateral post-operative x-rayImage courtesy of John M. Flynn, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Unstable SCFE of the right hip fixed with 2 screws. Left hip prophylactic fixation with a single screw. Frog-leg lateral post-operative x-rayImage courtesy of John M. Flynn, MD [Citation ends].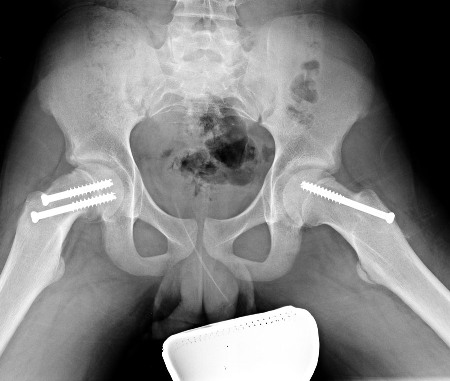
One accepted approach is to operate acutely, with percutaneous decompression of the hip joint, gentle repositioning of the slip, and fixation with screws or wires.[46] Early manipulative reduction of SCFE is recommended.
Open reduction and internal fixation with subcapital (intraarticular) osteotomy, with or without surgical hip dislocation, allows restoration of proximal femoral anatomy and may decrease the risk of avascular necrosis (AVN) in unstable SCFE. This procedure is associated with low complication rates in the hands of surgeons experienced with the technique.[40][41][42][47] Further long-term studies are needed to determine if it will be a better treatment long term gentle repositioning with decompression and screw fixation.
Open reduction is a technically demanding technique, and the variability of rates of AVN is such that clear audit of outcomes within any centre undertaking this procedure is advisable.[43][44]
Meta-analysis of 4 studies comparing outcomes in reduced or unreduced unstable slipped capital femoral epiphysis found no statistically significant difference in risk of AVN between treatment groups.[48] Meta-analysis of five studies that assessed timing of management found that treatment within 24 hours from the onset of instability was associated with a lower risk of AVN than treatment beyond that time.[48]
in situ screw fixation
In situ single-screw fixation is the widely accepted first-line treatment for SCFE.[37][38] The screw is placed in the centre of the epiphysis both on the antero-posterior and lateral aspects.[Figure caption and citation for the preceding image starts]: Unstable SCFE of the right hip fixed with 2 screws. Left hip prophylactic fixation with a single screw. Antero-posterior post-operative x-rayImage courtesy of John M. Flynn, MD [Citation ends].[Figure caption and citation for the preceding image starts]: Unstable SCFE of the right hip fixed with 2 screws. Left hip prophylactic fixation with a single screw. Frog-leg lateral post-operative x-rayImage courtesy of John M. Flynn, MD [Citation ends]. Advantages of in situ single-screw fixation include easy technique, low further slip rate, and prevention of complications.[39]
Alternative techniques, including in situ fixation with multiple screws, have also been described.[38] Post-operatively, toe-touch weight bearing is permitted for the first 2 weeks followed by weight bearing as tolerated.
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer