Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
bowel protection
Treatment recommended for ALL patients in selected patient group
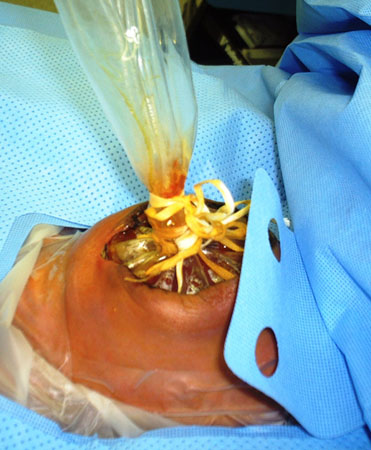
A sterile covering or a clear bowel bag should be placed immediately over the herniated abdominal contents to prevent evaporation, heat loss, and infection.
The infant should then be urgently transferred to a neonatal intensive unit with specialised paediatric surgical capacity.[32][Figure caption and citation for the preceding image starts]: Immediately after delivery, an infant with gastroschisis is placed in a protective bowel bagFrom collection of J.J. Tepas III, MD, FACS, FAAP [Citation ends].




Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer