Investigations
1st investigations to order
dermatoscopy
Test
Dermatoscopic patterns of melanocytic nevi vary depending on type, but generally show symmetrical structures and colours.[37][68] Nevi generally possess 1 or 2 colours, and the colours seen often reflect the location of the pigment in the skin. Black and brown colours indicate pigment in the epidermis, whereas grey or blue colours indicate pigment in the superficial and deep dermis, respectively.
Typical global patterns of melanocytic nevi seen with dermatoscopy include a reticular pattern, in which a grid of brown lines overlies a light brown background, and a globular pattern, with numerous brown, round-to-oval structures.
Other patterns include cobblestone (variation of globular pattern; papillomatous or mammillated dermal nevus), homogeneous pigment (diffuse grey-blue to grey-black pigmentation without other patterns; blue nevi), and starburst (pigmented streaks in a radial arrangement of the edge; Spitz nevi). Comedo-like follicular pseudo-openings may also be seen in nevi.
Dysplastic or Clark's nevi often have asymmetrical pink, brown, and tan coloration. The pigment network may be typical or atypical, with hypopigmented areas.
A multi-component pattern is a combination of 3 or more patterns and may signify a higher possibility of melanoma.
Other factors influence the dermatoscopic findings of melanocytic nevi.[69] Nevi located on special sites exhibit distinctive clinical, dermatoscopic, and histopathological features of which the clinician should be aware. For example, nevi of the face may show a pseudo-network pattern secondary to prominent follicular units, and acral nevi exhibit a parallel furrow pattern in which pigment is accentuated in the narrow furrows of the dermatoglyphs. Age, skin type, ultraviolet light exposure, pregnancy, and growth dynamics also influence the dermatoscopic findings of melanocytic nevi.[Figure caption and citation for the preceding image starts]: Dermatoscopy of a blue nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].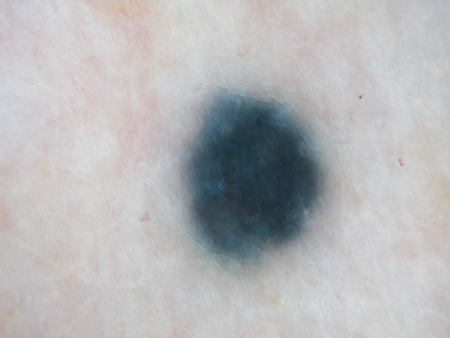 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a nevus with a reticular pigment networkFrom the collection of Laurel Schwartz, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a nevus with a reticular pigment networkFrom the collection of Laurel Schwartz, Thomas Jefferson University [Citation ends].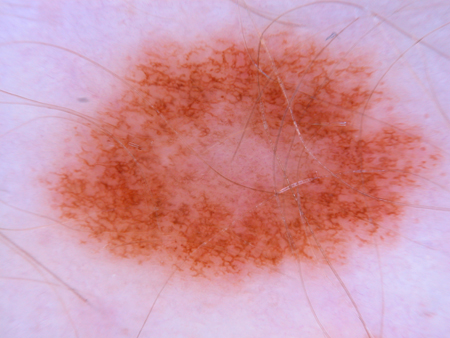 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a cobblestone pattern with a peripheral pigment networkFrom the collection of Jason B. Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a cobblestone pattern with a peripheral pigment networkFrom the collection of Jason B. Lee, Thomas Jefferson University [Citation ends].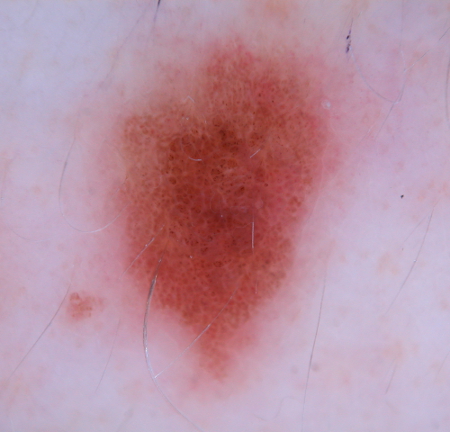 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a dysplastic or Clark's nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a dysplastic or Clark's nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].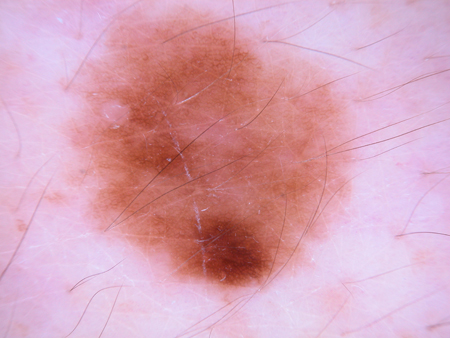 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a dysplastic or Clark's nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a dysplastic or Clark's nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].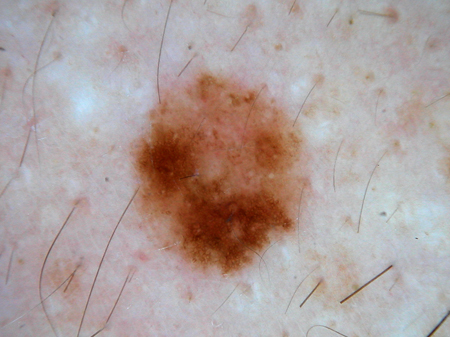 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a dysplastic or Clark's nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a dysplastic or Clark's nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].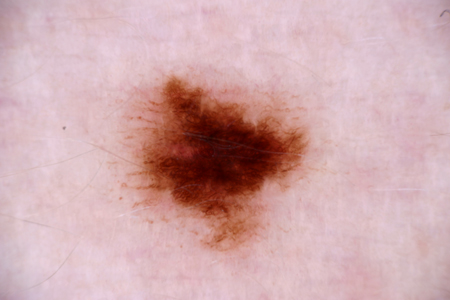 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a pigmented Spitz nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a pigmented Spitz nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].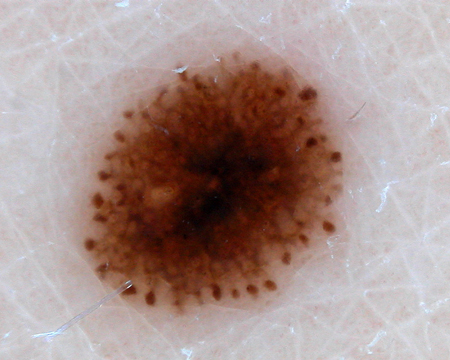 [Figure caption and citation for the preceding image starts]: Dermatoscopy of a volar nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: Dermatoscopy of a volar nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends]. [Figure caption and citation for the preceding image starts]: A volar nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
[Figure caption and citation for the preceding image starts]: A volar nevusFrom the collection of Jason Lee, Thomas Jefferson University [Citation ends].
Result
features of melanocytic nevi
Investigations to consider
non-invasive imaging technologies
Test
Several medical devices have been developed in an effort to aid primary-care physicians and dermatologists in their diagnostic accuracy of benign versus malignant pigmented melanocytic neoplasms. There are several different non-invasive imaging technologies available for research and clinical purposes. Optical generated techniques, such as optical coherence tomography (OCT) and confocal microscopy, differ from dermatoscopy or epiluminescence microscopy, which use multispectral imaging to provide visualisation of the horizontal plane.[39][40] Using a hand-held device to measure the light scatter of a neoplasm, these newer multispectral imaging techniques utilise computer-generated algorithms to determine the level of disorganisation, and thus malignant risk, of an individual lesion.
Result
features of melanocytic nevi versus melanoma
total body photography
Test
Some centres specialising in pigmented lesions utilise total body photography as an adjunct to help identify changes in nevi in an effort to detect melanomas at an earlier stage.[32]
In its ideal execution, this practice is reassuring to patient and physician, and may result in fewer benign nevi being excised. Limitations in this approach are that changes in nevi do not necessarily imply malignant transformation, as each nevus has a natural history over the patient's life.
Result
changes in melanocytic nevi
biopsy
Test
Most melanocytic nevi do not need to be removed; however, reasons for biopsy may be patient-driven, ranging from repetitive trauma to cosmetic concerns. Medically, suspicion of malignancy is the most important reason to biopsy a pigmented lesion. Melanomas are known to harbour chromosomal aberrations that are different from Spitz nevi and other melanocytic nevi. Aberrations in DNA copy number can be detected using fluorescent in-situ hybridisation (FISH) and comparative genomic hybridisation (CGH).[62] Immunohistochemistry may also be used to differentiate between nevi and melanoma. Application of PRAME (PReferentially expressed Antigen in MElanoma) immunohistochemical stain on ambiguous melanocytic lesions has been widely adopted by pathologists as most melanocytic nevi do not stain for this marker.[63]
Result
features of melanocytic nevi
Emerging tests
whole genome sequencing
Test
As molecular diagnostics continue to advance, additional diagnostic tools are emerging to assist in management and diagnosis of melanocytic lesions. Mutation in the TERT promoter gene is found in approximately 80% of melanomas. The presence of mutation in the TERT gene is helpful in differentiating melanoma from a nevus.[64]
Result
presence of mutation in the TERT gene
pigmented lesion assay (PLA)
Test
A non-invasive gene-profiling tape stripping test has been developed with a reported sensitivity of 95% and specificity of 60%, boasting a negative predictive value of 99%.[59] As a relatively new test that has not been independently validated, it is not widely utilised as of yet.
Result
positive for melanoma-associated genes PRAME and LINC00518 and the TERT mutation found in most melanomas
Use of this content is subject to our disclaimer