Once the source of the bleeding is identified, treatment may follow. Diagnostic methods may be often combined with treatment. Referral to a gastrointestinal surgeon and gastroenterologist is recommended during or after stabilisation.
Supportive care
After assessment of the patient's haemodynamic status (vital signs), depending on the degree of blood loss, the patient may need protection and support of the airway through intubation. The patient's circulatory status is assessed with attention to the degree of blood loss, blood pressure, and pulse.
Supportive care includes giving intravenous fluids and blood transfusions as indicated, and should continue as needed in haemodynamically stable patients. The European Society of Gastrointestinal Endoscopy recommends red blood cell transfusion in haemodynamically stable patients with acute lower gastrointestinal bleeding and no history of cardiovascular disease, with a haemoglobin threshold of ≤ 70 g/L (≤ 7 g/dL) prompting red blood cell transfusion.[38]Triantafyllou K, Gkolfakis P, Gralnek IM, et al. Diagnosis and management of acute lower gastrointestinal bleeding: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2021 Aug;53(8):850-68.
https://www.thieme-connect.com/products/ejournals/html/10.1055/a-1496-8969
http://www.ncbi.nlm.nih.gov/pubmed/34062566?tool=bestpractice.com
In those with a history of cardiovascular disease, a haemoglobin threshold of ≤ 80 g/L (≤ 8 g/dL) should prompt red blood cell transfusion.[38]Triantafyllou K, Gkolfakis P, Gralnek IM, et al. Diagnosis and management of acute lower gastrointestinal bleeding: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2021 Aug;53(8):850-68.
https://www.thieme-connect.com/products/ejournals/html/10.1055/a-1496-8969
http://www.ncbi.nlm.nih.gov/pubmed/34062566?tool=bestpractice.com
Haemodynamically unstable
In patients with unstable angiodysplastic bleeding, guidelines recommend CT angiography as the initial test to assess the arterial anatomy and localise the bleeding point.[18]Sengupta N, Kastenberg DM, Bruining DH, et al. The role of imaging for GI bleeding: ACG and SAR consensus recommendations. Radiology. 2024 Mar;310(3):e232298.
http://www.ncbi.nlm.nih.gov/pubmed/38441091?tool=bestpractice.com
[35]Sengupta N, Feuerstein JD, Jairath V, et al. Management of patients with acute lower gastrointestinal bleeding: an updated ACG guideline. Am J Gastroenterol. 2023 Feb 1;118(2):208-31.
https://journals.lww.com/ajg/fulltext/2023/02000/management_of_patients_with_acute_lower.14.aspx
http://www.ncbi.nlm.nih.gov/pubmed/36735555?tool=bestpractice.com
[38]Triantafyllou K, Gkolfakis P, Gralnek IM, et al. Diagnosis and management of acute lower gastrointestinal bleeding: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2021 Aug;53(8):850-68.
https://www.thieme-connect.com/products/ejournals/html/10.1055/a-1496-8969
http://www.ncbi.nlm.nih.gov/pubmed/34062566?tool=bestpractice.com
This should be followed by mesenteric angiography with a view to embolisation to control the source of bleeding.[34]Karuppasamy K, Kapoor BS, Fidelman N, et al. Expert panel on interventional radiology, ACR appropriateness criteria® radiologic management of lower gastrointestinal tract bleeding: 2021 update. J. Am. Coll. Radiol. 2021 May 21;18(5):S139-52.
https://www.jacr.org/article/S1546-1440(21)00153-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/33958109?tool=bestpractice.com
[39]Raju GS, Gerson L, Das A, et al. American Gastroenterological Association (AGA) Institute medical position statement on obscure gastrointestinal bleeding. Gastroenterology. 2007 Nov;133(5):1697-717.
http://www.gastrojournal.org/article/S0016-5085%2807%2901148-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/17983812?tool=bestpractice.com
An upper gastrointestinal endoscopy may be performed next to rule out a source proximal to the distal duodenum.
Colonoscopy or surgery may be appropriate in the absence of angiography. During colonoscopy, electrocautery, photocoagulation, clips, or an adrenaline (epinephrine) injection may be indicated to treat the lesion. For patients with colonic angiodysplasias, careful treatment in the right colon is recommended, due to the thinner walls and higher risk for perforation. For patients with recurrent small bowel bleeding, endoscopic management via device-assisted enteroscopy can be considered depending on the patient’s clinical course and response to prior therapy.[8]Gerson LB, Fidler JL, Cave DR, et al. ACG clinical guideline: diagnosis and management of small bowel bleeding. Am J Gastroenterol. 2015 Sep;110(9):1265-87; quiz 1288.
https://journals.lww.com/ajg/fulltext/2015/09000/acg_clinical_guideline__diagnosis_and_management.10.aspx
http://www.ncbi.nlm.nih.gov/pubmed/26303132?tool=bestpractice.com
Electrocautery uses heated probes to coagulate the bleeding lesions. Photocoagulation uses argon and Yag lasers and requires specific training. Argon photocoagulation appears to be safe and effective in patients with bleeding from colonic angiodysplasia.[62]Olmos JA, Marcolongo M, Pogorelsky V, et al. Long-term outcome of argon plasma ablation therapy for bleeding in 100 consecutive patients with colonic angiodysplasia. Dis Colon Rectum. 2006 Oct;49(10):1507-16.
https://www.doi.org/10.1007/s10350-006-0684-1
http://www.ncbi.nlm.nih.gov/pubmed/17024322?tool=bestpractice.com
[63]Olmos JA, Marcolongo M, Pogorelsky V, et al. Argon plasma coagulation for prevention of recurrent bleeding from GI angiodysplasias. Gastrointest Endosc. 2004 Dec;60(6):881-6.
https://www.doi.org/10.1016/s0016-5107(04)02221-7
http://www.ncbi.nlm.nih.gov/pubmed/15605001?tool=bestpractice.com
[64]Pichon Riviere A, Augustovski F, Garcia Marti S, et al. Argon plasma usefulness for the treatment of gastrointestinal lesions. Buenos Aires, Argentina: Ciudad de Buenos Aires, Institute for Clinical Effectiveness and Health Policy (IECS); 2005.[Figure caption and citation for the preceding image starts]: Endoscopic (device-assisted enteroscopy) image of small bowel angiodysplasia after treatment with argon plasma coagulationFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].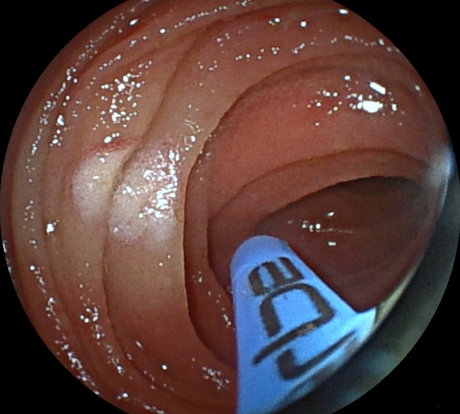 [Figure caption and citation for the preceding image starts]: Endoscopic image of argon plasma coagulation of colonic angiodysplasiaPermission obtained from patient; GNU Free Documentation License [Citation ends].
[Figure caption and citation for the preceding image starts]: Endoscopic image of argon plasma coagulation of colonic angiodysplasiaPermission obtained from patient; GNU Free Documentation License [Citation ends]. Capsule endoscopy may also be indicated in a specific group where the above investigations have not yielded a source of bleeding. There may be a role for device-assisted enteroscopy after a positive capsule endoscopy to treat a small bowel bleeding lesion.
Capsule endoscopy may also be indicated in a specific group where the above investigations have not yielded a source of bleeding. There may be a role for device-assisted enteroscopy after a positive capsule endoscopy to treat a small bowel bleeding lesion.
[Figure caption and citation for the preceding image starts]: Small bowel angiodysplasia seen during small bowel capsule endoscopyFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].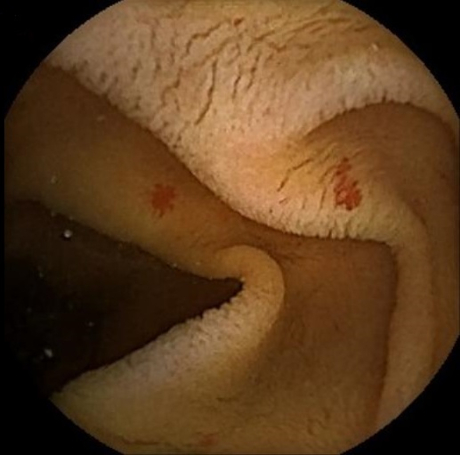 [Figure caption and citation for the preceding image starts]: Small bowel angiodysplasia seen during small bowel capsule endoscopyFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Small bowel angiodysplasia seen during small bowel capsule endoscopyFrom the personal collection of Dr Elli, Milan, Italy; used with permission [Citation ends].
Only patients with a large, life-threatening haemorrhage with little relief from interventional endoscopy or embolisation are appropriate for surgery. At operation, the patient may undergo an on-table enteroscopy to localise the bleeding before a blind sub-total colectomy. Ideally, the bleed site should be identified before resection. Recurrent bleeding is still common after right hemicolectomy, as unidentified lesions may still be present. Aortic valve replacement should be considered in patients with Heyde’s syndrome, known small bowel angiodysplasia, and ongoing bleeding.[8]Gerson LB, Fidler JL, Cave DR, et al. ACG clinical guideline: diagnosis and management of small bowel bleeding. Am J Gastroenterol. 2015 Sep;110(9):1265-87; quiz 1288.
https://journals.lww.com/ajg/fulltext/2015/09000/acg_clinical_guideline__diagnosis_and_management.10.aspx
http://www.ncbi.nlm.nih.gov/pubmed/26303132?tool=bestpractice.com
As surgery carries a high mortality, consider it only when all other options are exhausted.
Haemodynamically stable
If the patient has a stable airway and vital signs, most bleeding episodes will stop spontaneously.
An elective colonoscopy is recommended to identify the source of bleeding. During the procedure, electrocautery, photocoagulation, clips, or an adrenaline injection may be indicated to treat the lesion.[34]Karuppasamy K, Kapoor BS, Fidelman N, et al. Expert panel on interventional radiology, ACR appropriateness criteria® radiologic management of lower gastrointestinal tract bleeding: 2021 update. J. Am. Coll. Radiol. 2021 May 21;18(5):S139-52.
https://www.jacr.org/article/S1546-1440(21)00153-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/33958109?tool=bestpractice.com
If the endoscopy is negative and the bleeding continues, based on local expertise, capsule endoscopy or CT angiography should be performed which may guide further intervention. If CT angiography confirms active bleeding, it should be followed by a mesenteric angiography with a view to embolisation to treat the bleeding.[39]Raju GS, Gerson L, Das A, et al. American Gastroenterological Association (AGA) Institute medical position statement on obscure gastrointestinal bleeding. Gastroenterology. 2007 Nov;133(5):1697-717.
http://www.gastrojournal.org/article/S0016-5085%2807%2901148-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/17983812?tool=bestpractice.com
Device-assisted enteroscopy can be used to treat bleeding lesions in the small bowel, seen on CT or capsule endoscopy.
If device-assisted enteroscopy or angiography is unavailable or unsuccessful and the patient is a surgical candidate, surgery can be considered. Surgery should not be used as a diagnostic tool to localise the site of bleeding in haemodynamically stable patients.[34]Karuppasamy K, Kapoor BS, Fidelman N, et al. Expert panel on interventional radiology, ACR appropriateness criteria® radiologic management of lower gastrointestinal tract bleeding: 2021 update. J. Am. Coll. Radiol. 2021 May 21;18(5):S139-52.
https://www.jacr.org/article/S1546-1440(21)00153-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/33958109?tool=bestpractice.com
The exact procedure used will depend on the likely site(s) of the bleeding based on preoperative and intraoperative investigations.
If the patient is inappropriate for surgery, drug therapy is an option, but minimal research supports usage and results are mixed.[39]Raju GS, Gerson L, Das A, et al. American Gastroenterological Association (AGA) Institute medical position statement on obscure gastrointestinal bleeding. Gastroenterology. 2007 Nov;133(5):1697-717.
http://www.gastrojournal.org/article/S0016-5085%2807%2901148-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/17983812?tool=bestpractice.com
One systematic review and meta-analysis found that pharmacological treatment of any kind led to significantly reduced bleeding episodes and notable improvement in haemoglobin levels.[65]Gkolfakis P, Fostier R, Tziatzios G, et al. Efficacy of pharmacologic treatment for treating gastrointestinal angiodysplasias-related bleeding: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2022 Oct 1;34(10):1021-30.
http://www.ncbi.nlm.nih.gov/pubmed/35913758?tool=bestpractice.com
Somatostatin analogues (e.g., octreotide, lanreotide) and thalidomide have shown benefit in this setting. There is poor evidence for oestrogen derivatives.[39]Raju GS, Gerson L, Das A, et al. American Gastroenterological Association (AGA) Institute medical position statement on obscure gastrointestinal bleeding. Gastroenterology. 2007 Nov;133(5):1697-717.
http://www.gastrojournal.org/article/S0016-5085%2807%2901148-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/17983812?tool=bestpractice.com
[66]Brown C, Subramanian V, Wilcox CM, et al. Somatostatin analogues in the treatment of recurrent bleeding from gastrointestinal vascular malformations: an overview and systematic review of prospective observational studies. Dig Dis Sci. 2010 Aug;55(8):2129-34.
http://www.ncbi.nlm.nih.gov/pubmed/20393879?tool=bestpractice.com
[67]Swanson E, Mahgoub A, MacDonald R, et al. Medical and endoscopic therapies for angiodysplasia and gastric antral vascular ectasia: a systematic review. Clin Gastroenterol Hepatol. 2014 Apr;12(4):571-82.
https://www.doi.org/10.1016/j.cgh.2013.08.038
http://www.ncbi.nlm.nih.gov/pubmed/24013107?tool=bestpractice.com
One multi-centre randomised controlled trial found that octreotide reduced transfusion requirements and the annual volume of endoscopic procedures in patients with angiodysplasia-related anaemia.[68]Goltstein LCMJ, Grooteman KV, Bernts LHP, et al. Standard of care versus octreotide in angiodysplasia-related bleeding (the OCEAN study): a multicenter randomized controlled trial. Gastroenterology. 2024 Apr;166(4):690-703.
https://www.gastrojournal.org/article/S0016-5085(23)05685-8/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/38158089?tool=bestpractice.com
Long-term lanreotide therapy has shown to significantly improve anaemia and reduce hospitalisations, blood transfusions, and endoscopies in patients with angiodysplasias.[69]Frago S, Alcedo J, Martín Pena-Galo E, et al. Long-term results with lanreotide in patients with recurrent gastrointestinal angiodysplasias bleeding or obscure gastrointestinal bleeding. Benefits in efficacy and procedures consumption. Scand J Gastroenterol. 2018 Dec;53(12):1496-502.
http://www.ncbi.nlm.nih.gov/pubmed/30621520?tool=bestpractice.com
[70]Hawks MK, Svarverud JE. Acute lower gastrointestinal bleeding: evaluation and management. Am Fam Physician. 2020 Feb 15;101(4):206-12.
https://www.aafp.org/pubs/afp/issues/2020/0215/p206.html
http://www.ncbi.nlm.nih.gov/pubmed/32053333?tool=bestpractice.com
Systematic reviews suggest that somatostatin analogue therapy is safe and effective in patients with gastrointestinal angiodysplasia; octreotide therapy may be more effective than lanreotide therapy.[71]Jackson CS, Gerson LB. Management of gastrointestinal angiodysplastic lesions (GIADs): a systematic review and meta-analysis. Am J Gastroenterol. 2014 Apr;109(4):474-83.
https://www.ncbi.nlm.nih.gov/books/NBK196085
http://www.ncbi.nlm.nih.gov/pubmed/24642577?tool=bestpractice.com
[72]Goltstein LCMJ, Grooteman KV, Rocco A, et al. Effectiveness and predictors of response to somatostatin analogues in patients with gastrointestinal angiodysplasias: a systematic review and individual patient data meta-analysis. Lancet Gastroenterol Hepatol. 2021 Nov;6(11):922-32.
https://www.doi.org/10.1016/S2468-1253(21)00262-4
http://www.ncbi.nlm.nih.gov/pubmed/34508668?tool=bestpractice.com
One retrospective study reported that somatostatin analogue therapy plus endoscopic therapy reduced bleeding episodes in patients with recurrent anaemia and small bowel angioectasia.[46]Tai FWD, Chetcuti-Zammit S, Sidhu R. Small bowel angioectasia-the clinical and cost impact of different management strategies. Clin Res Hepatol Gastroenterol. 2023 Oct;47(8):102193.
http://www.ncbi.nlm.nih.gov/pubmed/37553067?tool=bestpractice.com
Re-bleeding
If re-bleeding occurs, a repeat capsule endoscopy may be appropriate to localise site of bleeding before further intervention.[35]Sengupta N, Feuerstein JD, Jairath V, et al. Management of patients with acute lower gastrointestinal bleeding: an updated ACG guideline. Am J Gastroenterol. 2023 Feb 1;118(2):208-31.
https://journals.lww.com/ajg/fulltext/2023/02000/management_of_patients_with_acute_lower.14.aspx
http://www.ncbi.nlm.nih.gov/pubmed/36735555?tool=bestpractice.com