Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
activity modification and physiotherapy
Patients should be advised to avoid exacerbating activities in order to interrupt the cycle of ongoing inflammation. This may mean that pain control and avoidance of physiotherapy are necessary in the early painful stages of treatment.
Physiotherapy is the cornerstone of successful treatment of adhesive capsulitis, and should be initiated as early as possible in the disease course.
A home exercise regimen, consisting of both active and passive range of motion exercises, combined with formal supervised outpatient therapy is optimal once pain control is achieved.[38]
Preliminary findings from a systematic review of 7 different mobilisation techniques have shown that the Maitland technique (a high-grade mobilisation technique) and combined mobilisations have beneficial effects. However, more research is needed to determine the most successful mobilisation technique.[40]
Addition of treatment modalities such as iontophoresis (electrical pulse activity), phonophoresis (ultrasound therapy), and cryotherapy may be of some benefit. However, evidence supporting their success is not clear.[41]
A useful exercise that can be performed at the patient's home and with the therapist is known as the sleeper stretch, which works on improving internal rotation. In the lateral decubitus position (patient on side), with the affected shoulder down against the bed, the elbow is flexed 90° and the unaffected arm pushes it towards the bed. [Figure caption and citation for the preceding image starts]: Demonstration of sleeper stretch exerciseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
activity modification and physiotherapy
Treatment recommended for ALL patients in selected patient group
Patients should be advised to avoid exacerbating activities in order to interrupt the cycle of ongoing inflammation. This may mean that pain control and avoidance of physiotherapy are necessary in the early painful stages of treatment.
Physiotherapy is the cornerstone of successful treatment of adhesive capsulitis, and should be initiated as early as possible in the disease course.
A home exercise regimen, consisting of both active and passive range of motion exercises, combined with formal supervised outpatient therapy is optimal once pain control is achieved.[38]
Preliminary findings from a systematic review of 7 different mobilisation techniques have shown that the Maitland technique (a high-grade mobilisation technique) and combined mobilisations have beneficial effects. However, more research is needed to determine the most successful mobilisation technique.[40]
Addition of treatment modalities such as iontophoresis (electrical pulse activity), phonophoresis (ultrasound therapy), and cryotherapy may be of some benefit. However, evidence supporting their success is not clear.[41]
A useful exercise that can be performed at the patient's home and with the therapist is known as the sleeper stretch, which works on improving internal rotation. In the lateral decubitus position (patient on side), with the affected shoulder down against the bed, the elbow is flexed 90° and the unaffected arm pushes it towards the bed. [Figure caption and citation for the preceding image starts]: Demonstration of sleeper stretch exerciseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
activity modification and physiotherapy
Treatment recommended for ALL patients in selected patient group
Patients should be advised to avoid exacerbating activities in order to interrupt the cycle of ongoing inflammation. This may mean that pain control and avoidance of physiotherapy are necessary in the early painful stages of treatment.
Physiotherapy is the cornerstone of successful treatment of adhesive capsulitis, and should be initiated as early as possible in the disease course.
A home exercise regimen, consisting of both active and passive range of motion exercises, combined with formal supervised outpatient therapy is optimal once pain control is achieved.[38]
Preliminary findings from a systematic review of 7 different mobilisation techniques have shown that the Maitland technique (a high-grade mobilisation technique) and combined mobilisations have beneficial effects. However, more research is needed to determine the most successful mobilisation technique.[40]
Addition of treatment modalities such as iontophoresis (electrical pulse activity), phonophoresis (ultrasound therapy), and cryotherapy may be of some benefit. However, evidence supporting their success is not clear.[41]
A useful exercise that can be performed at the patient's home and with the therapist is known as the sleeper stretch, which works on improving internal rotation. In the lateral decubitus position (patient on side), with the affected shoulder down against the bed, the elbow is flexed 90° and the unaffected arm pushes it towards the bed. [Figure caption and citation for the preceding image starts]: Demonstration of sleeper stretch exerciseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
activity modification and physiotherapy
Treatment recommended for ALL patients in selected patient group
Patients should be advised to avoid exacerbating activities in order to interrupt the cycle of ongoing inflammation. This may mean that pain control and avoidance of physiotherapy are necessary in the early painful stages of treatment.
Physiotherapy is the cornerstone of successful treatment of adhesive capsulitis, and should be initiated as early as possible in the disease course.
A home exercise regimen, consisting of both active and passive range of motion exercises, combined with formal supervised outpatient therapy is optimal once pain control is achieved.[38]
Preliminary findings from a systematic review of 7 different mobilisation techniques have shown that the Maitland technique (a high-grade mobilisation technique) and combined mobilisations have beneficial effects. However, more research is needed to determine the most successful mobilisation technique.[40]
Addition of treatment modalities such as iontophoresis (electrical pulse activity), phonophoresis (ultrasound therapy), and cryotherapy may be of some benefit. However, evidence supporting their success is not clear.[41]
A useful exercise that can be performed at the patient's home and with the therapist is known as the sleeper stretch, which works on improving internal rotation. In the lateral decubitus position (patient on side), with the affected shoulder down against the bed, the elbow is flexed 90° and the unaffected arm pushes it towards the bed. [Figure caption and citation for the preceding image starts]: Demonstration of sleeper stretch exerciseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
arthroscopic capsular release
Over time, arthroscopy has come to play an essential role in the surgical treatment of refractory adhesive capsulitis.
Arthroscopic release of the anterior capsule, rotator interval, and/or release of the coracohumeral ligament provides improvement in pain and function.[18][63][64][65] Both short-term and long-term benefits have been shown.[18][66][67] A posterior capsular release may be considered with loss of internal rotation despite adequate physiotherapy and stretching. Release of the intra-articular portion of the subscapularis tendon and/or an extended release of the inferior glenohumeral ligament from inferior to posterior may improve range of motion, but only short-term results are available.[68][69]
The use of arthroscopic release is being considered earlier in the course of the disease. However, optimal timing of surgical intervention has yet to be defined.[Figure caption and citation for the preceding image starts]: Arthroscopic view of contracted anterior capsule with extensive synovitis and thickeningFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].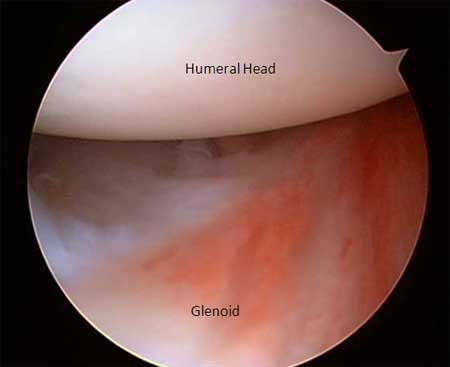 [Figure caption and citation for the preceding image starts]: Arthroscopic view of completed anterior releaseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic view of completed anterior releaseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].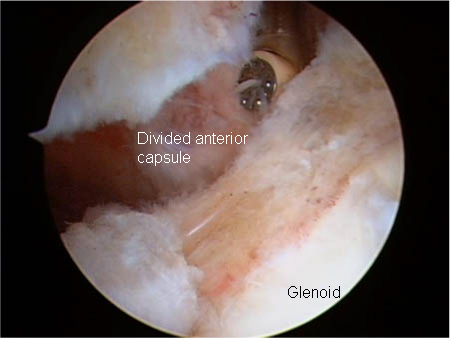 [Figure caption and citation for the preceding image starts]: Arthroscopic view of contracted rotator interval showing extensive scarring and synovitisFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic view of contracted rotator interval showing extensive scarring and synovitisFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].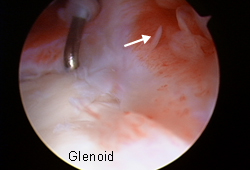 [Figure caption and citation for the preceding image starts]: Arthroscopic view of rotator interval releaseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic view of rotator interval releaseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].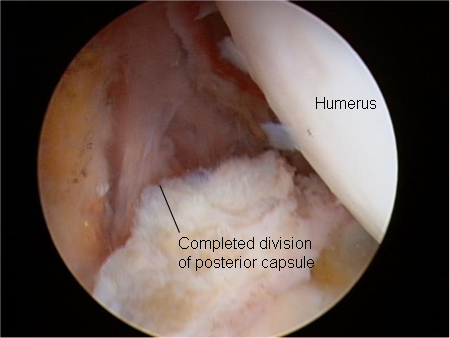 [Figure caption and citation for the preceding image starts]: Arthroscopic view of posterior capsular releaseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Arthroscopic view of posterior capsular releaseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].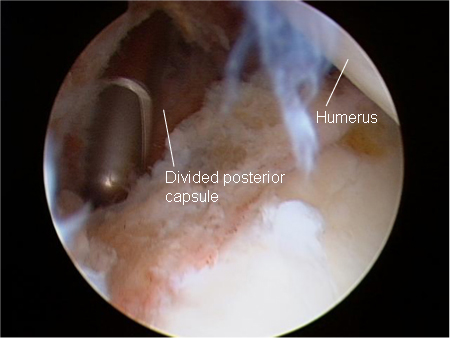
activity modification and physiotherapy
Treatment recommended for ALL patients in selected patient group
Patients should be advised to avoid exacerbating activities in order to interrupt the cycle of ongoing inflammation. This may mean that pain control and avoidance of physiotherapy are necessary in the early painful stages of treatment.
Physiotherapy is the cornerstone of successful treatment of adhesive capsulitis, and should be initiated as early as possible in the disease course.
A home exercise regimen, consisting of both active and passive range of motion exercises, combined with formal supervised outpatient therapy is optimal once pain control is achieved.[38]
Preliminary findings from a systematic review of 7 different mobilisation techniques have shown that the Maitland technique (a high-grade mobilisation technique) and combined mobilisations have beneficial effects. However, more research is needed to determine the most successful mobilisation technique.[40]
Addition of treatment modalities such as iontophoresis (electrical pulse activity), phonophoresis (ultrasound therapy), and cryotherapy may be of some benefit. However, evidence supporting their success is not clear.[41]
A useful exercise that can be performed at the patient's home and with the therapist is known as the sleeper stretch, which works on improving internal rotation. In the lateral decubitus position (patient on side), with the affected shoulder down against the bed, the elbow is flexed 90° and the unaffected arm pushes it towards the bed. [Figure caption and citation for the preceding image starts]: Demonstration of sleeper stretch exerciseFrom the private collection of Matthew T. Provencher, MD, CDR MC USN and Lance E. LeClere, MD, LCDR MC USN; used with permission [Citation ends].
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer