Aetiology
Ductal carcinoma in situ (DCIS) is a non-invasive breast cancer that is confined to the duct in which it originated and does not extend beyond the basement membrane.[1] The terminal duct lobular unit is the origin of most lesions. DCIS is part of a continuum of progression from benign disease to invasive cancer, which includes typical hyperplasia, atypical hyperplasia, DCIS, and invasive breast cancer.[23]
Similarly to invasive breast cancer, approximately two-thirds of DCIS specimens express oestrogen receptor, with the fraction of tumours expressing oestrogen receptor depending on the degree of differentiation.[6] HER2, a cell surface marker in the epidermal growth factor family that is used to guide therapy of invasive breast cancer, is expressed in both DCIS and invasive breast cancer, with higher rates of expression in DCIS.[24][25] A variety of other markers are differentially expressed in DCIS and invasive breast cancer compared with benign breast disease, including p53, vascular endothelial growth factor, and cyclin D1.[6]
Oestrogen levels, which are higher in women than in men, stimulate proliferation of breast epithelial cells in the lobules and ducts. Spontaneous mutations in epithelial cells, some of which provide a survival advantage to the cell, lead to precancerous changes. Further mutations lead to in situ or invasive breast cancer.[26]
Pathophysiology
Breast cancer in situ comprises ductal carcinoma in situ (DCIS), a non-invasive breast cancer that is confined to the duct in which it originates, and lobular carcinoma in situ (LCIS), a neoplastic proliferation of cells in the breast lobule(s) and/or terminal ducts.
Ductal carcinoma in situ (DCIS)
Microarrays have been used to investigate the association of DCIS and invasive breast cancer. There were greater associations seen between low-grade DCIS and low-grade invasive disease and high-grade DCIS and high-grade invasive disease, than between low- and high-grade DCIS.[6] This suggests that low-grade DCIS may progress to low-grade invasive cancer, and high-grade DCIS to high-grade invasive cancer.
Lobular carcinoma in situ (LCIS)
LCIS develops in breast lobule(s) and/or terminal ducts and is usually found incidentally. LCIS is not cancer but a pathological description of a neoplastic proliferation of cells within lobules and/or terminal ducts, which is a risk factor for invasive breast cancer.[5] A finding of LCIS does not imply that cancer will form at the site where it is found. Studies suggest an association between classic LCIS and bilateral cancer risk, but not consistently.[27][28][29] Treatment for LCIS is less formalised than for DCIS.[Figure caption and citation for the preceding image starts]: Lobular carcinoma in situFrom the private collection of Dr Sauter; used with permission [Citation ends].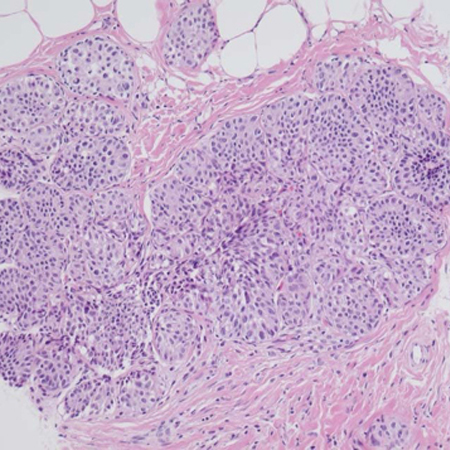
Pleomorphic and florid LCIS are often associated with the concomitant presence of DCIS and invasive breast cancer.[30][31] Recurrence appears to be lower when there are clear margins of >2 mm and adjuvant radiation is administered. Level 1 evidence (from a systematic review or meta-analysis) for pleomorphic and florid LCIS treatment is lacking.
Classification
Architectural classification of ductal carcinoma in situ (DCIS)[6]
Pathological analysis is necessary to determine the histological subtype. Architectural subtypes of DCIS are comedo and non-comedo. The comedo subtype is characterised by prominent apoptotic cell death and has greater malignant potential than non-comedo subtypes.[7] Non-comedo subtypes are further subdivided: the classification is descriptive, and there are no consistently associated clinical implications.
Comedo
Non-comedo
Cribriform
Micropapillary
Papillary
Solid
Clinging.
Use of this content is subject to our disclaimer