History and exam
Key diagnostic factors
common
presence of risk factors
Risk factors include infections (group A beta-haemolotyic streptococci, hepatitis B and C, respiratory and gastrointestinal infections, infective endocarditis, HIV), connective tissue diseases (systemic lupus erythematosus, systemic vasculitides), malignancy (lung cancer, colorectal cancer, Hodgkin's lymphoma, non-Hodgkin's lymphoma, leukaemia, thymoma), haemolytic uraemic syndrome, and drugs.
haematuria
Microscopic haematuria is common; haematuria that is visible to the patient has variable frequency depending on the type of GN.
oedema
Generalised. More specific to nephrotic syndrome.
hypertension
Reduced estimated estimated glomerular filtration rate (eGFR) together with salt and water retention results in systemic hypertension.
Other diagnostic factors
common
oliguria
Early presentation if kidney failure develops rapidly, otherwise a late feature.
anorexia
Part of a generalised vasculitic picture.
nausea
Part of a generalised vasculitic picture.
malaise
Part of a generalised vasculitic picture.
weight loss
May indicate systemic disease.
fever
May occur with infectious aetiology: for example, post-streptococcal GN.
skin rash
In vasculitic aetiology.[Figure caption and citation for the preceding image starts]: Palpable purpura on the lower extremities of a child with IgA vasculitis (Henoch-Schonlein purpura)From the collection of Dr Paul F. Roberts [Citation ends].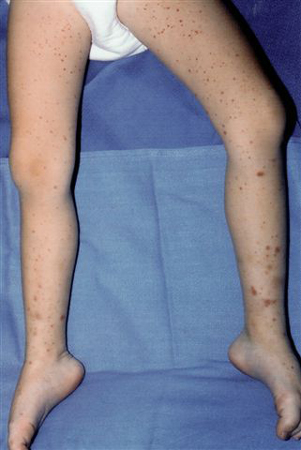
arthralgia
In vasculitic aetiology.
haemoptysis
In anti-glomerular basement membrane disease and granulomatosis with polyangiitis, and rarely in systemic lupus erythematosus.
abdominal pain
In post-streptococcal GN and IgA vasculitis (Henoch-Schonlein purpura).
sore throat
Preceding renal symptoms by 1-2 weeks in post-streptococcal GN and at the same time in IgA nephropathy.
uncommon
hypervolaemia
Symptoms of fluid overload due to reduced urinary output, such as shortness of breath and oedema.
Risk factors
strong
group A beta-haemolytic Streptococcus
Nephrogenic Streptococcus pyogenes strains 12, 4, and 1 are associated with post-streptococcal GN triggered by throat infections, whereas S pyogenes M types 49, 42, 2, 57, and 60 are linked to post-streptococcal GN triggered by skin infections.[9] The incidence of clinically detectable disease in children infected with pharyngitis is approximately 5% to 10%, and the incidence of skin infections during an epidemic is 25%.[27]
respiratory infections
May trigger recurrent episodes of gross haematuria, beginning within 1-3 days of infection.[28]
gastrointestinal infections
May trigger recurrent episodes of gross haematuria, beginning 1-3 days post-infection.[28]
hepatitis B
Can result in the deposition of circulating antigen-antibody complexes in the mesangium and subendothelial space (causing membranoproliferative pattern of glomerular injury), in the subepithelial space (causing membranous nephropathy and nephrotic syndrome), or in the vessels (causing polyarteritis nodosa).[29]
hepatitis C
The most common patterns of renal involvement are membranoproliferative pattern of glomerular injury (with cryoglobulinaemia) and, frequently, membranous nephropathy. The pathogenesis appears to relate to deposition of immune complexes containing antibodies to the virus and viral RNA in the glomeruli.[30]
infective endocarditis
Common organisms are Staphylococcus aureus and Streptococcus viridans. There is immune complex deposition in the subendothelium and subepithelium, as well as thickening of the capillary wall. Patients with endocarditis-associated GN from organisms with low virulence (e.g., S viridans), mostly present with a membranoproliferative pattern of glomerular injury.[9]
HIV
A collapsing form of focal segmental glomerulosclerosis has been considered the primary form of HIV nephropathy, especially in black people. The mechanisms by which these changes occur are not well understood, but may be related to direct infection of the glomerulus by HIV.
Proliferative GN, immunoglobulin A (IgA) nephropathy, and lupus-like GN have also been described. Other presentations due to co-infection with hepatitis B or C, concurrent intravenous drug use, and therapy-related GN may also occur.[31][32]
systemic lupus erythematosus (SLE)
Renal involvement is common in idiopathic SLE, with the prevalence of clinically evident renal disease ranging from 40% to 75%. The time course for the development of lupus nephritis varies with sex, age, and ethnicity. It appears that males, younger patients, and non-white Americans are at increased risk of developing nephritis earlier in the course of the disease. The pattern and extent of glomerular injury is primarily related to the site of formation of the immune deposits and is accordingly classified into 6 different patterns or classes.[33]
systemic vasculitis
Such as classic polyarteritis nodosa, granulomatosis with polyangiitis, microscopic polyarteritis, eosinophilic granulomatous polyangiitis (Churg-Strauss syndrome), and the hypersensitivity vasculitides (including IgA vasculitis [Henoch-Schonlein purpura], mixed cryoglobulinaemia, and serum sickness).[34]
lung cancer
Solid tumours are associated with membranous nephropathy. The likely mechanism is deposition of tumour antigens within the glomeruli, followed by antibody deposition and complement activation.[35]
colorectal cancer
Solid tumours are associated with membranous nephropathy. The likely mechanism is deposition of tumour antigens within the glomeruli, followed by antibody deposition and complement activation.[35]
Hodgkin's lymphoma
Minimal change disease mostly occurs at the time of initial presentation, whereas focal glomerulosclerosis may occur as a late event.[36]
non-Hodgkin's lymphoma
A wide spectrum of renal lesions can be observed in patients with non-Hodgkin lymphoma, including a membranoproliferative glomerulonephritis-like pattern and minimal change disease.[37]
leukaemia
Minimal change disease, focal glomerulosclerosis, or membranoproliferative pattern of glomerular injury may occur in association with leukaemia.[38]
thymoma
Minimal change disease or focal glomerulosclerosis may occur in association with thymoma.[35]
haemolytic uraemic syndrome
Has been associated with membranoproliferative pattern of glomerular injury.[35]
drugs
Well-studied offending agents include gold sodium thiomalate, hydralazine, lithium, propylthiouracil, and non-steroidal anti-inflammatory drugs.[39]
Use of this content is subject to our disclaimer