Approach
Most neural tube defects are detected antenatally or at birth. The physical examination should include careful documentation of cranial nerve and cerebellar functioning, manual muscle strength testing and deep tendon reflexes, sensory level, presence of anal wink, and rectal tone.
Investigations such as cranial ultrasound, computed tomography (CT) of head, and magnetic resonance imaging (MRI) of head and cervical spine are required if hydrocephalus or underlying structural anatomical abnormalities are suspected. These baseline data are essential for patient management during acute illnesses. Any deterioration from baseline should be evaluated promptly with a high index of suspicion for progressive hydrocephalus or shunt malfunction (if present).
Antenatal history
Spina bifida and anencephaly are typically diagnosed by antenatal ultrasound and are rarely a diagnostic challenge. Ultrasound examination in the second and third trimester can be beneficial for the screening of fetal anomalies; however, significant variability in the sensitivity of routine ultrasonography for detection of fetal anomalies has been reported. The benefits and limitations of ultrasonography should be discussed with all patients.[71]
Family and maternal history should focus on the presence of any mid-line congenital anomalies that may suggest an underlying chromosomal disorder (e.g., conotruncal heart defects, renal anomalies, cleft lip, or cleft palate) or unexplained pregnancy loss.
Antenatal history should focus on known risk factors, including exposure to potential teratogens (e.g., valproic acid and its derivatives, carbamazepine, isotretinoin, or methotrexate), maternal nutritional status (including vitamin supplementation, particularly folic acid), and presence of maternal diabetes. It is important to ascertain whether or not amniocentesis has been offered and if limb deformities or cardiac or renal anomalies have been documented on the antenatal ultrasound. If present, these findings warrant a genetic work-up, high-resolution ultrasound, and/or fetal MRI (fast MRI of the fetus can be used to better define structural brain anomalies that may be associated with some neural tube defects).[61][72][73][74]
Parents may be overwhelmed with information, or misinformed about the diagnosis. Therefore, their understanding of the diagnosis and prognosis should also be explored as part of the antenatal visit.
Antenatal assessment
Antenatal assessment with the quadruple screen, which includes AFP (alpha-fetoprotein), hCG, uE3 (unconjugated estriol), and inhibin A, is routinely offered between 15 and 22 weeks' gestation. A mathematical calculation involving the levels of these substances and considerations of maternal age, weight, race, and diabetic status are used to determine risk. The quadruple screen can detect about 75% to 80% of pregnancies affected by spina bifida and nearly 95% of those with anencephaly.[60][75]
Ultrasound following an elevated quadruple screen excludes an open neural tube defect with a high degree of confidence, although interpretation requires a great deal of expertise, and false-negative studies have been reported.[60][61][76][77]
When a fetus is identified as having a neural tube defect, amniocentesis should be offered in order to identify associated chromosome abnormalities, specifically trisomy 13 and trisomy 18. The identification of a genetic abnormality has important implications for counselling regarding prognosis, pregnancy management, and assessing whether the patient is a candidate for in-utero neural tube defect repair.[60][78][79][80] Chromosome micro-array and/or whole exome trio testing, as well as genetic counselling, is offered if there are multiple congenital anomalies.[61][81]
Fetal echocardiography may be considered if antenatal ultrasound suggests a congenital cardiac malformation, or a genetic syndrome associated with cardiac defects is suspected. If fetal echocardiography or family history is suggestive of velocardiofacial syndrome, fluorescence in situ hybridisation (FISH) testing to identify micro-deletion of 22q11 is also indicated.
Fetal MRI may be performed if antenatal fetal surgery is being considered or if there are unclear findings on ultrasonography.[60][61][78][82] The absence of a covering membrane is associated with scoliosis and high-risk bladder dysfunction.[83][84]
Newborn and infancy
History
Shortly after birth and during early infancy it is important to ask about the presence of feeding difficulties, which can be related to weakness in brainstem innervated muscles; symptoms of hydrocephalus including arching of the neck or stridulous cry, rapid head growth, bulging of the fontanelle, downward deviation of the eyes (sunsetting); and whether or not asymmetry has been noted in the baby's spontaneous movement of the arms and legs.
Stooling and voiding patterns should also be discussed as neurogenic bladder and bowel are common features, although the latter is rarely a problem in infancy. Infants should wet a minimum of 4 nappies in a 24-hour period. A distended bladder and decreased urine output suggests incomplete emptying. Constant urinary dribbling suggests an open bladder outlet, overflow incontinence, or an ectopic ureter. Oozing of stool suggests low anal sphincter tone. Constipation is unusual in the neonatal period.
Difficulty with changing the nappy or dressing should be established. This may indicate decreased range of motion in the legs or the presence of spasticity.
Hindbrain herniation is present at birth in approximately two-thirds of infants who have undergone antenatal closure of the myelomeningocele and nearly all (96%) infants who undergo postnatal closure.[85][86][87] This consists of caudal displacement of the cerebellar tonsils and vermis, caudal medulla, and occasionally the fourth ventricle, into the cervical spinal canal. Some infants may also have associated findings such as dysgenesis of corpus callosum and abnormalities of neuronal migration and brain sulcation. These findings are associated with an increased risk for learning disability. Symptoms related to the hindbrain herniation are a clinical concern for 15% to 35% of patients and can be life-threatening in the first 3 months of life.[86][88] These include choking, nasal regurgitation, vomiting, reflux, aspiration pneumonias, apnoea, arching of the neck, snoring, inspiratory stridor, and a hoarse or high-pitched cry.
Physical examination
Lesions that are not covered by skin are termed open spina bifida. Types include the following.
Myelomeningocele: herniation of both meninges and spinal cord. Associated with hydrocephalus and Chiari II malformation.
Meningocele: herniation of the meninges without involvement of spinal elements. [Figure caption and citation for the preceding image starts]: Neonate with myelomeningoceleFrom the collection of Dr Greg Liptak; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: MyelomeningoceleFrom the collection of Dr Greg Liptak; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: MyelomeningoceleFrom the collection of Dr Greg Liptak; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: MeningoceleFrom the collection of Dr Zulma Tovar-Spinoza; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: MeningoceleFrom the collection of Dr Zulma Tovar-Spinoza; used with permission [Citation ends].
Lesions that are covered by skin are termed closed spina bifida. They are usually associated with a visible abnormality of the back, such as asymmetrical gluteal fold or dimple, haemangioma, hairy patch, or other cutaneous markings. [Figure caption and citation for the preceding image starts]: MyelomeningocystoceleFrom the collection of Dr Zulma Tovar-Spinoza; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: Skin tagFrom the collection of Dr Zulma Tovar-Spinoza; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Skin tagFrom the collection of Dr Zulma Tovar-Spinoza; used with permission [Citation ends].
Growth parameters should be monitored, including daily head circumference and fontanelle size. Rapid head growth (crossing of 2 percentile categories) and bulging of the fontanelle indicate progressive hydrocephalus.
Inspection for major or minor congenital anomalies should be performed, particularly mid-line congenital anomalies such as cleft lip or palate and cardiac murmur. These findings, if present, should prompt genetic evaluation for trisomy 13, trisomy 18, and 22q deletion syndrome if not already tested antenatally.
Facial asymmetry and other cranial nerve abnormalities, including upward and lateral gaze deviation, palate elevation, weak suck, and high-pitched cry, are signs of raised intracranial pressure and symptomatic Chiari II malformation that require close monitoring by a neurosurgeon.
The presence of any orthopaedic deformities should be assessed, including congenital scoliosis, congenital kyphosis, subluxed or dislocated hips (as demonstrated by asymmetrical hip abduction, or positive Barlow's or Ortolani's sign: eliciting a clunk from the hip as it relocates), knee and hip flexion contractures, club foot (equinovarus deformity), and vertical talus (rigid rocker-bottom flat foot).
Position of the newborn or infant at rest and volitional movement when alert should be noted, including abdominal muscle control. Muscle tone and bulk in upper and lower extremities should be evaluated as well as presence of anal wink and rectal tone. Tone varies depending on the level of the lesion. Dribbling of urine or leakage of meconium or stool suggests decreased bladder sphincter tone and rectal tone, respectively. Sensory function is often decreased and should be assessed by checking pinprick sensation in the feet, legs, and buttocks, which is demonstrated by reduced or absent response to pinprick.
Investigations
Cranial ultrasound is used in cases of suspected hydrocephalus to estimate cortical mantle thickness and monitor progression of ventricle size prior to shunt placement. Asymptomatic infants who have stable mild or moderate ventriculomegaly may be monitored safely for up to 5 months as long as cortical mantle thickness is at least 3.5 cm on cranial ultrasound.
Spinal ultrasound is recommended in neonates with lumbosacral stigmata known to be associated with spinal dysraphism, such as midline or paramedian masses and/or neurocutaneous markings (e.g., hypertrichosis, haemangiomas), pinpoint midline dimples, and paramedian deep dimples. Ultrasound may reveal defects such as tethering, diastomyelia, hydromyelia, or syringomyelia.[89]
Cranial imaging (ultrasound, MRI, or CT) may also be performed after shunt insertion to confirm ventriculoperitoneal catheter placement. Low radiation techniques should be used when available, and repeated CT exposure should be avoided.
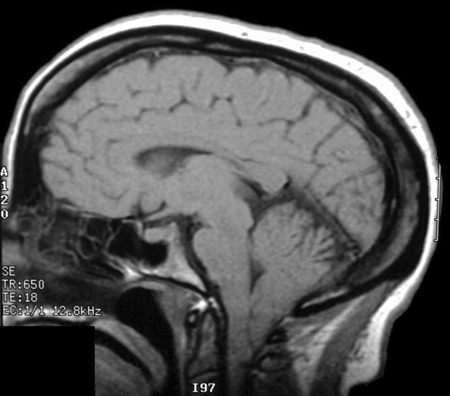
MRI scan is used to evaluate structural brain anomalies such as agenesis of corpus callosum. MRI is indicated if Chiari symptoms are severe or if the neurological examination is markedly asymmetrical. These symptoms warrant close follow-up by the neurosurgeon and MRI imaging of the head and cervical spine to evaluate for progressive hydrocephalus and/or an associated syringomyelia (extension of the central canal with obstruction and cyst formation in the spinal cord, known as a syrinx). Chiari malformation is the caudal displacement of the cerebellar tonsils and vermis, caudal medulla, and occasionally the fourth ventricle, into the cervical spinal canal. [Figure caption and citation for the preceding image starts]: Brain MRI scan showing Chiari malformationFrom the collection of Dr Nienke P. Dosa; used with permission [Citation ends].
Urine culture should be obtained in all newborns with spina bifida. In the first 2 months of life, bacteriuria, even if asymptomatic, should be treated. This is because urinary tract infection can be difficult to diagnose in neonates, it can rapidly progress to sepsis, and there is a greater risk of renal cortical scarring in the neonatal period compared with older age groups.
Serum creatinine and urea should be obtained once the infant is more than 5 days old. Earlier studies reflect maternal levels. If urea and creatinine are elevated, intermittent catheterisation is started and a urologist and nephrologist consulted.
Renal and bladder ultrasound should be obtained several days after the cele repair to determine kidney size and configuration, to estimate bladder capacity, and to evaluate for presence of hydronephrosis.
Urodynamic study is recommended between 6 and 12 months of age to determine detrusor leak-point pressure and presence of detrusor sphincter dyssynergia, as well as bladder capacity and compliance. This information guides management of neurogenic bladder.
Voiding cystourethrogram (VCUG) is performed only if the renal ultrasound shows hydronephrosis, to identify whether vesicoureteral reflux is present and antibiotic prophylaxis is indicated. Some centres prefer to perform a urodynamic study at 4-6 weeks of age for this purpose.[90][91][92] However, not all centres are able to perform urodynamic studies in neonates; many will just perform a renal and bladder ultrasound plus a VCUG to assess bladder function at this stage.
Chromosome testing for trisomy 18 and trisomy 13 and FISH testing for 22q deletion syndrome are indicated (if not already done antenatally) if the newborn examination documents other major congenital anomalies or if there are more than 3 minor congenital anomalies in addition to spina bifida.
Hip ultrasound is obtained for infants 3 months of age or younger, with sacral motor levels (likely to be ambulatory), who have asymmetrical hip abduction or positive Barlow's or Ortolani's sign (eliciting a clunk from the hip as it relocates). Beyond 3 months of age, conventional x-ray studies are used to evaluate the hips. There is controversy about whether imaging is needed for children with higher lesion levels, because treatment is of little benefit and there is a high risk of re-dislocation in non-ambulatory children.
Polysomnography should be considered across the lifespan of the patient to identify Chiari-related sleep-disordered breathing such as central sleep apnoea and hypoventilation.[93][94]
Use of this content is subject to our disclaimer