Approach
A detailed history and a thorough physical examination should enable the diagnosis to be elucidated in most patients with seronegative arthritis. Supporting or confirmatory data are obtained from laboratory and imaging studies.[39]
History
The number and location of joints involved (monoarticular versus polyarticular), the mode of onset (acute versus continuous and progressive), and the characteristics of joint involvement provide clues to the aetiology of the arthritis.
Key features
Articular pain: may present abruptly or as a gradual discomfort. When symptoms last more than 6 weeks, the condition is regarded as chronic. It is necessary to determine whether the joint involvement occurred simultaneously, in an additive fashion (pain persists in one or more joints and spreads to involve other joints), or in a migratory fashion (pain persists in one or more joints then disappears in the initially involved joints and spreads to involve other joints).
Joint involvement: establishing whether joint involvement is symmetrical or asymmetrical is also important. Both peripheral joint involvement and axial symptoms should be ascertained.
Morning stiffness: the presence of early morning stiffness lasting >1 hour suggests inflammatory arthritis.[40][41]
Inflammatory back pain: insidious onset of low back pain in a patient <35-45 years of age with a positive family history of spondyloarthropathy, that worsens in the second-half of the night, eases with exercise and non-steroidal anti-inflammatory drugs (NSAIDs), and is associated with alternating buttock pain and early morning stiffness of ≥1 hour, may be suggestive of underlying axial spondyloarthropathy.[42][43][44][45][46][47]
Other key features of the history
Constitutional symptoms: such as fever, suggestive of systemic processes or infection. A thorough review of systems should elicit extra-articular features.
Infection: characteristic risk factors for infectious monoarthritis should be sought, including age over 80 years, diabetes mellitus, rheumatoid arthritis, joint surgery, hip or knee prosthesis, skin infection, and human immunodeficiency infection.[15][16][17][18]
Medical history: a family history of spondyloarthropathy, history of uveitis, psoriasis, inflammatory bowel disease, urethritis, and sexually transmitted diseases should be considered in patients with suspected spondyloarthropathies. If gout is suspected, a history of podagra (inflammation of the great toe) should be sought, although it may not be present in women with polyarticular gout. History of tick or mosquito bites, travel, and illness of children or pets should be considered. Chikungunya virus arthritis should be considered with a travel history to, or residence in, an endemic area, especially if the symptoms have an acute onset.[39][48][49]
Physical examination
Key features of the examination
Joint examination: in order to narrow the differential diagnoses, it is important to document the presence of synovitis and the distribution of involvement. Viral arthropathies rarely cause effusions directly. If dactylitis is present, spondyloarthropathies should be considered.
Spine examination: in patients with long-standing spondyloarthropathy, restriction of range of motion (ROM) of the spine may be noted. A Schober's test may be conducted by placing a measuring tape 10 cm apart at the midline in the lower lumbar spine. The patient is asked to aim to touch his or her toes without bending the knees. Normally, lumbar spine flexion would result in an excursion of 5 cm or more. If the excursion is <4 cm, it may be significant for restriction of ROM of the lumbar spine due to syndesmophyte formation.
Skin changes: a careful dermatological examination should be conducted to elicit signs of psoriasis, erythema nodosum, keratoderma blennorrhagicum, purpura, cutaneous manifestations of connective tissue disease (alopecia, discoid lesions, malar rash, serpiginous eruption, Gottron's papules, truncal eruption of dermatomyositis), and hand features of scleroderma (sclerodactyly, skin thickening, digital pits or ulcers, Raynaud's phenomenon, abnormal nail-fold capillaroscopy, subcutaneous calcinosis). Rashes may be associated with viral arthritis. A maculopapular, morbilliform rash, hyperpigmentation, and intertriginous lesions may occur in chikungunya virus infection.
Lymphadenopathy: seen in systemic disorders or infection.
Muscle weakness: proximal muscle weakness may suggest inflammatory myopathy.
Mononeuritis multiplex: seen in vasculitis or systemic lupus erythematosus.
Pleuropericarditis or pleural effusion: may suggest connective tissue disease.[Figure caption and citation for the preceding image starts]: Psoriasis plaque: legsFrom the collection of Dr Tsu-Yi Chuang; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: Erythema nodosum on the shin of a patientFrom the collection of Dr Om P. Sharma; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Erythema nodosum on the shin of a patientFrom the collection of Dr Om P. Sharma; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Keratoderma blennorrhagica in a patient with reactive arthritisImage provided by the CDC Public Health Image Library [Citation ends].
[Figure caption and citation for the preceding image starts]: Keratoderma blennorrhagica in a patient with reactive arthritisImage provided by the CDC Public Health Image Library [Citation ends]. [Figure caption and citation for the preceding image starts]: Macular erythematous patches (Gottron's papules) over the toes with dystrophic cuticlesAdapted from BMJ Case Reports 2009 [doi:10.1136/bcr.06.2009.2027] Copyright © 2009 by the BMJ Publishing Group Ltd [Citation ends].
[Figure caption and citation for the preceding image starts]: Macular erythematous patches (Gottron's papules) over the toes with dystrophic cuticlesAdapted from BMJ Case Reports 2009 [doi:10.1136/bcr.06.2009.2027] Copyright © 2009 by the BMJ Publishing Group Ltd [Citation ends]. [Figure caption and citation for the preceding image starts]: Hand demonstrating sclerodactyly with finger curling, shiny skin at the fingers, and telangiectasiasFrom the collection of Maureen D. Mayes; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Hand demonstrating sclerodactyly with finger curling, shiny skin at the fingers, and telangiectasiasFrom the collection of Maureen D. Mayes; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Digital pits without ulcersFrom the collection of Maureen D. Mayes; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Digital pits without ulcersFrom the collection of Maureen D. Mayes; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Hands demonstrating Raynaud's phenomenonFrom the collection of Maureen D. Mayes; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Hands demonstrating Raynaud's phenomenonFrom the collection of Maureen D. Mayes; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Late-stage sclerodactyly with contractures due to severe skin tighteningFrom the collection of Maureen D. Mayes; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Late-stage sclerodactyly with contractures due to severe skin tighteningFrom the collection of Maureen D. Mayes; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Diffuse hyperaemia or erythroderma during the acute phase of chikungunya virus infectionFrom the collection of Dr Fabrice Simon; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Diffuse hyperaemia or erythroderma during the acute phase of chikungunya virus infectionFrom the collection of Dr Fabrice Simon; used with permission [Citation ends].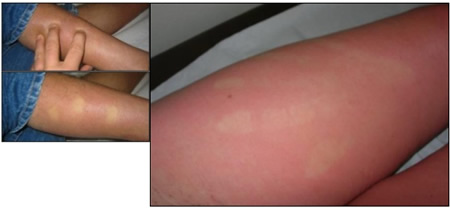 [Figure caption and citation for the preceding image starts]: Diffuse morbilliform rash during the acute phase of chikungunya virus infectionFrom the collection of Dr Fabrice Simon; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Diffuse morbilliform rash during the acute phase of chikungunya virus infectionFrom the collection of Dr Fabrice Simon; used with permission [Citation ends].
Features of spondyloarthropathies
Axial spondyloarthritis (ankylosing spondylitis) presents in patients aged 20-30 years and has a male-to-female ratio of 3:1.[50][51] It shows familial aggregation, and HLA-B27 is present in 90% of patients.[52] Clinically it manifests with asymmetrical lower extremity arthritis, symmetrical sacroiliitis, and delicate marginal syndesmophytes (initially involving the lumbar and lower thoracic spine). Uveitis occurs occasionally, while enthesitis and dactylitis are uncommon, and dermatological manifestations are non-specific. Other extra-articular manifestations are aortic regurgitation, conduction defects, upper lobe pulmonary fibrosis, and IgA nephropathy.[Figure caption and citation for the preceding image starts]: Plain radiograph showing bilateral sacroiliitis in a patient with ankylosing spondylitisBMJ 2006;333:581-585. Copyright@2009 by the BMJ Publishing Group [Citation ends].

Reactive arthritis presents in patients aged 20-40 years. Both sexes are equally affected; however, reactive arthritis caused by Chlamydia trachomatis has a greater male predominance.[53] Reactive arthritis shows familial aggregation, and the prevalence in patients positive with HLA-B27 is 5-10 times higher than the general population.[54] Clinically it manifests with asymmetrical lower extremity arthritis, asymmetrical sacroiliitis, and bulky syndesmophytes. Uveitis, enthesitis, and dactylitis are common, and dermatological manifestations of keratoderma blennorrhagicum and circinate balanitis occur. Aortic regurgitation is another extra-articular manifestation.[Figure caption and citation for the preceding image starts]: Keratoderma blennorrhagica in a patient with reactive arthritisImage provided by the CDC Public Health Image Library [Citation ends].
Psoriatic arthritis presents in patients aged 40-50 years and occurs equally in men and women.[55] People who have a first-degree relative with psoriatic arthritis are 40 times more likely to develop the disease.[56] Twin and family studies, human leukocyte antigen (HLA), and genome-wide scans have implicated multiple genetic influences.[57] It can involve any peripheral joint and causes asymmetrical sacroiliitis, as well as bulky marginal syndesmophytes (commonly in the cervical spine). Uveitis occurs occasionally, while enthesitis and dactylitis are common, and dermatologically it manifests with psoriasis. Aortic regurgitation is another extra-articular manifestation.[Figure caption and citation for the preceding image starts]: Psoriatic arthritisFrom the collection of Dr Tsu-Yi Chuang; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: Psoriasis plaque: legsFrom the collection of Dr Tsu-Yi Chuang; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Psoriasis plaque: legsFrom the collection of Dr Tsu-Yi Chuang; used with permission [Citation ends].Enteropathic arthritis presents in patients aged 25-45 years and occurs equally in men and women.[58] It shows familial aggregation, and HLA-B27 is frequently present in the axial form of enteropathic arthritis (compared to the peripheral form) in about 50% to 75% of patients.[59] Clinically it manifests with asymmetrical lower extremity arthritis, symmetrical sacroiliitis, and delicate marginal syndesmophytes. Enthesitis occurs less commonly, dactylitis is uncommon, and uveitis occurs occasionally. Dermatological manifestations of erythema nodosum and pyoderma gangrenosum. Aortic regurgitation can also occur. [Figure caption and citation for the preceding image starts]: Erythema nodosum on the shin of a patientFrom the collection of Dr Om P. Sharma; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Features of spondyloarthropathiesAdapted from Kataria RK, Brent LH. Am Fam Physician. 2004;69:2853-2260 and Gladman DD. Am J Med Sci.1998;316:234-238 [Citation ends].
Discriminating features in polyarthritis
Fever preceding the arthritis indicates the possibility of viral arthritis, Lyme arthritis, reactive arthritis, juvenile- or adult-onset idiopathic arthritis, or bacterial endocarditis. A temperature >40°C (>104°F) may indicate juvenile- or adult-onset idiopathic arthritis, bacterial arthritis, or systemic lupus erythematosus (SLE).
A migratory pattern of arthritis occurs in rheumatic fever, disseminated gonococcal or meningococcal infection, viral arthritis, and SLE. Episodic recurrences occur in Lyme disease, crystal-induced arthritis, enteropathic arthritis, Whipple's disease, juvenile- or adult-onset idiopathic arthritis, and SLE.
Pain out of proportion with the degree of effusion indicates the possibility of rheumatic fever, acute leukaemia, or AIDS, while the presence of a large effusion with less pain may indicate tuberculous arthritis, sub-acute bacterial endocarditis, enteropathic arthritis, giant cell arteritis, or Lyme disease.
Leukopenia may be present in SLE and viral arthritis.
[Figure caption and citation for the preceding image starts]: Discriminating features in polyarthritisAdapted from Pinals R. N Engl J Med. 1994;330:769-774 [Citation ends].
Diagnostic tests
The laboratory and imaging assessment should be focused towards the suspected diagnosis.
Suspected multisystemic involvement
Full blood count with differential, comprehensive metabolic profile, urinalysis, C-reactive protein, and erythrocyte sedimentation rate should be performed. A chest x-ray may also be helpful for the identification of underlying conditions such as tuberculosis and sarcoidosis. [Figure caption and citation for the preceding image starts]: Bilateral hilar adenopathyFrom the collection of Muthiah P. Muthiah, MD, FCCP; used with permission [Citation ends].

Suspected rheumatoid arthritis
Cyclic citrullinated peptide antibodies may be drawn in a patient with symmetrical polyarthritis. Although its specificity is high for rheumatoid arthritis, it may also occur in psoriatic arthritis and may denote a worse prognosis.[60][61]
Suspected connective tissue disease
Initial work-up includes antinuclear antibodies and Sjogren's syndrome A and Sjogren's syndrome B antibodies.
Suspected spondyloarthropathy
HLA-B27 measurement on its own is generally not useful because it has poor predictive value for spondyloarthropathy in the general population.[62] However, in combination with clinical and radiological findings, it may increase diagnostic confidence and aid the early diagnosis of axial spondyloarthropathy.[45][46]
Plain x-rays may be helpful in detecting erosions or specific signs of a disease process. However, in early arthritis, bony changes may not be detected, limiting their usefulness.[63][64] The hallmark of spondyloarthropathy is spine involvement. Syndesmophyte formation and signs of sacroiliitis may be seen. In patients with psoriatic arthritis, x-rays may detect marginal erosions, which are generally indistinguishable from those of rheumatoid arthritis. However, they tend to have an asymmetrical distribution affecting the carpus, metacarpophalangeal, and interphalangeal (IP) joints. The upper extremity is involved more often than lower extremities. In the lower extremities, IP joint erosions are common. Periosteal new bone formation, distal interphalangeal joint erosion, or pencil-in-cup deformities may also be observed.[65]
If axial spondyloarthropathy is suspected, and sacroiliac joint x-rays are negative, magnetic resonance imaging (MRI) of the sacrum may be utilised to detect active inflammation, tissue metaplasia, and erosions at the ilium.[66] MRI of the spine may detect increased bone marrow signal and fatty metaplasia at the vertebral bodies. The prognostic and predictive value of MRI in this setting is unclear and European League Against Rheumatism guidelines do not recommend routine imaging of the spine for case finding.[66][67][68]
Sonography is more sensitive than physical examination in detecting signs of synovitis, tenosynovitis, and enthesitis.[39] It may play a role in classifying early inflammatory arthropathy, as well as detecting peripheral enthesitis.[63][66][69][70] It may also detect erosions and periostitis in these patients.[71][72]
Delayed diagnosis is associated with worse outcomes in patients with axial spondyloarthropathy.[73][74] The Assessment of Spondyloarthritis International Society working group has proposed and validated new classification criteria for axial spondyloarthritis that aim to identify patients earlier and not fully rely on radiographic changes in the spine or sacroiliac joint.[75] Studies have reported increased incidence of spondyloarthropathy based on these classification criteria.[76][77][78] However, only a proportion of these patients may progress to having radiographic evidence of spondyloarthropathy.[75]
Suspected rheumatic fever
Evidence of recent streptococcal infection may be sought by throat swabs or anti-streptolysin O titres. However, the sensitivity of these tests may be low, and anti-DNase B and anti-streptokinase titres may need to be obtained.[26]
Suspected infection
Joint aspiration is important to exclude infection.[79] However, crystalline arthropathies can co-exist with infectious arthritis.[80]
Synovial biopsy of a joint may be indicated if an infectious or granulomatous disorder is suspected, such as tuberculosis. However, it may not be useful for the diagnosis or prognostication of non-infectious peripheral arthritis.[81]
Suspected viral arthritis
Specific viral serologies may be performed based on the clinical presentation. In middle-aged women with acute polyarthritis, parvovirus IgG/IgM may be sought.
If chikungunya arthritis is suspected, IgG and IgM antibodies may be ordered.
Polymerase chain reaction for hepatitis B or C, HIV, or chikungunya virus may be ordered if the relevant antibodies are detected.
A minority of patients with chikungunya arthropathy may develop chronic symptoms. These patients should be evaluated for development of rheumatoid arthritis as well as other seronegative arthropathies according to their clinical characteristics. Rarely an erosive arthropathy may develop that is negative for rheumatoid factor and positive for anti-CCP antibodies.[82][Figure caption and citation for the preceding image starts]: Plain radiograph showing bilateral sacroiliitis in a patient with ankylosing spondylitisBMJ 2006;333:581-585. Copyright@2009 by the BMJ Publishing Group [Citation ends].
Suspected crystalline arthropathy
The diagnosis may be made by joint aspiration and recognising tophaceous deposits at the helix of the ear or extensor surfaces of the fingers.
Uric acid levels are often checked in patients with suspected gout, although they may be normal in an acute flare.[83]
Joint aspiration is helpful when gout or calcium pyrophosphate deposition disease (CPPD) is suspected.[79] Synovial fluid should be aspirated and intracellular CPPD crystals demonstrated.[84]
A diagnosis of tophaceous gout may be suggested by classic erosions with overhanging edges in plain x-rays.[85] The presence of chondrocalcinosis at the triangular fibrocartilage or menisci of knees is suggestive of CPPD. Synovial calcification may also be seen at the metacarpophalangeal joints, metatarsophalangeal joints, wrist, and knees. Synovial fluid examination under plane polarised microscopy is required to confirm the diagnosis.[86]
Sonography may be helpful in the diagnosis of crystalline arthropathy due to the differential deposition of urate and calcium pyrophosphate crystals in cartilage.[87] Tophaceous deposits may also be recognised.[87]
Although MRI shows active synovitis, the appearances of gout are not unique, limiting the usefulness of this technique in the diagnosis of crystalline arthropathy.[85][88][Figure caption and citation for the preceding image starts]: Chronic tophaceous gout showing nodules in periarticular structures and arthritisAdapted from BMJ Case Reports 2009 [doi:10.1136/bcr.03.2009.1668] Copyright © 2009 by the BMJ Publishing Group Ltd [Citation ends].
 [Figure caption and citation for the preceding image starts]: Knee radiograph with linear calcific deposits of cartilage calcificationFrom the collection of Ann K. Rosenthal, MD; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Knee radiograph with linear calcific deposits of cartilage calcificationFrom the collection of Ann K. Rosenthal, MD; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Wrist radiograph from a patient with chronic calcium pyrophosphate arthritis showing severe degenerative changesFrom the collection of Ann K. Rosenthal, MD; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Wrist radiograph from a patient with chronic calcium pyrophosphate arthritis showing severe degenerative changesFrom the collection of Ann K. Rosenthal, MD; used with permission [Citation ends].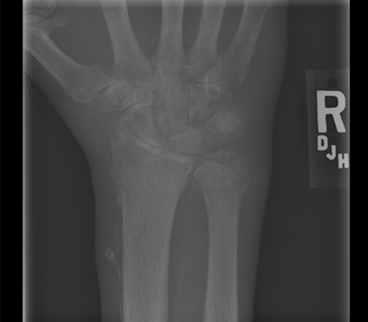 [Figure caption and citation for the preceding image starts]: Image of intracellular calcium pyrophosphate crystals under compensated polarising light microscopyFrom the collection of Ann K. Rosenthal, MD; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Image of intracellular calcium pyrophosphate crystals under compensated polarising light microscopyFrom the collection of Ann K. Rosenthal, MD; used with permission [Citation ends].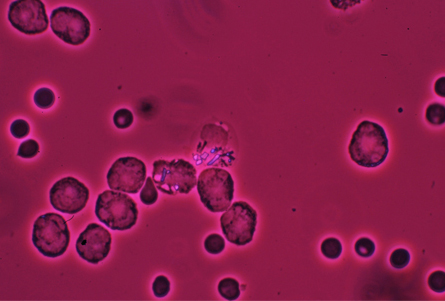
Use of this content is subject to our disclaimer