The majority of patients afflicted with epicondylitis will have complete resolution of their symptoms with arm rest and non-steroidal anti-inflammatory drug (NSAID) therapy.[4]Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994 Jan;2(1):1-8.
http://www.ncbi.nlm.nih.gov/pubmed/10708988?tool=bestpractice.com
[24]Ciccotti MG, Ramani MN. Medial epicondylitis. Tech Hand Up Extrem Surg. 2003 Dec;7(4):190-6.
http://www.ncbi.nlm.nih.gov/pubmed/16518220?tool=bestpractice.com
[56]Ciccotti MG, Charlton WP. Epicondylitis in the athlete. Clin Sports Med. 2001 Jan;20(1):77-93.
http://www.ncbi.nlm.nih.gov/pubmed/11227710?tool=bestpractice.com
Additional therapy may be required if there is no improvement after 6 weeks, or if symptoms are refractory to treatment.
Initial presentation
The mainstay of initial treatment for medial and lateral epicondylitis is rest, ice, and activity modification of the wrist, elbow, and forearm for 6 weeks.[1]Carter RM. Epicondylitis. J Bone Joint Surg Am. 1925;7:553-62.[4]Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994 Jan;2(1):1-8.
http://www.ncbi.nlm.nih.gov/pubmed/10708988?tool=bestpractice.com
[24]Ciccotti MG, Ramani MN. Medial epicondylitis. Tech Hand Up Extrem Surg. 2003 Dec;7(4):190-6.
http://www.ncbi.nlm.nih.gov/pubmed/16518220?tool=bestpractice.com
[57]Johnson GW, Cadwallader K, Scheffel SB, et al. Treatment of lateral epicondylitis. Am Fam Physician. 2007 Sep 15;76(6):843-8.
http://www.ncbi.nlm.nih.gov/pubmed/17910298?tool=bestpractice.com
Oral NSAIDs are recommended during the initial 10-21 days following injury. Short-term studies have demonstrated that oral diclofenac for 28 days is associated with improved pain in lateral epicondylitis, but does not statistically improve grip strength.[58]Pattanittum P, Turner T, Green S, et al. Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst Rev. 2013;(5):CD003686.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003686.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/23728646?tool=bestpractice.com
[59]Labelle H, Guibert R. Efficacy of diclofenac in lateral epicondylitis of the elbow also treated with immobilization. The University of Montreal Orthopaedic Research Group. Arch Fam Med. 1997 May-Jun;6(3):257-62.
http://www.ncbi.nlm.nih.gov/pubmed/9161352?tool=bestpractice.com
In addition to NSAIDs, an inelastic, non-articular, proximal forearm strap for lateral epicondylitis may be used. Short-term use of this bracing technique (counterforce bracing) for up to 12 weeks after injury has been shown to be beneficial.[60]Kroslak M, Pirapakaran K, Murrell GAC. Counterforce bracing of lateral epicondylitis: a prospective, randomized, double-blinded, placebo-controlled clinical trial. J Shoulder Elbow Surg. 2019 Feb;28(2):288-295.
https://www.doi.org/10.1016/j.jse.2018.10.002
http://www.ncbi.nlm.nih.gov/pubmed/30658774?tool=bestpractice.com
There is no difference in symptom improvement using a counterforce brace confined to a forearm compared with a brace with a strap above the elbow.[61]Bisset LM, Collins NJ, Offord SS. Immediate effects of 2 types of braces on pain and grip strength in people with lateral epicondylalgia: a randomized controlled trial. J Orthop Sports Phys Ther. 2014 Feb;44(2):120-8.
http://www.ncbi.nlm.nih.gov/pubmed/24405258?tool=bestpractice.com
Conservative treatment should be continued for about 6 weeks.
The use of transcutaneous electrical nerve stimulation (TENS) devices does not appear to provide additional benefit.[62]Chesterton LS, Lewis AM, Sim J, et al. Transcutaneous electrical nerve stimulation as adjunct to primary care management for tennis elbow: pragmatic randomised controlled trial (TATE trial). BMJ. 2013 Sep 2;347:f5160.
http://www.bmj.com/content/347/bmj.f5160
http://www.ncbi.nlm.nih.gov/pubmed/23999980?tool=bestpractice.com
No response to initial treatment at 6 weeks
If the patient fails to improve with rest, NSAIDs, and bracing, the physical examination should be repeated to re-evaluate for other aetiological processes. Radiographic and/or electrophysiological studies may also be indicated to further evaluate the patient.
Formal physiotherapy procedures, with or without local injections of local anaesthetic, may be beneficial and should include an eccentric loading programme.[63]Herd CR, Meserve BB. A systematic review of the effectiveness of manipulative therapy in treating lateral epicondylalgia. J Man Manip Ther. 2008;16(4):225-37.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2716156
http://www.ncbi.nlm.nih.gov/pubmed/19771195?tool=bestpractice.com
[64]Raman J, MacDermid JC, Grewal R. Effectiveness of different methods of resistance exercises in lateral epicondylosis - a systematic review. J Hand Ther. 2012 Jan-Mar;25(1):5-25.
http://www.ncbi.nlm.nih.gov/pubmed/22075055?tool=bestpractice.com
[65]Cullinane FL, Boocock MG, Trevelyan FC. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin Rehabil. 2014 Jan;28(1):3-19.
http://www.ncbi.nlm.nih.gov/pubmed/23881334?tool=bestpractice.com
[66]Olaussen M, Holmedal O, Lindbaek M, et al. Treating lateral epicondylitis with corticosteroid injections or non-electrotherapeutical physiotherapy: a systematic review. BMJ Open. 2013 Oct 29;3(10):e003564.
http://bmjopen.bmj.com/content/3/10/e003564.long
http://www.ncbi.nlm.nih.gov/pubmed/24171937?tool=bestpractice.com
[67]Peterson M, Butler S, Eriksson M, et al. A randomized controlled trial of eccentric vs. concentric graded exercise in chronic tennis elbow (lateral elbow tendinopathy). Clin Rehabil. 2014 Sep;28(9):862-72.
http://www.ncbi.nlm.nih.gov/pubmed/24634444?tool=bestpractice.com
[68]McQueen KS, Powell RK, Keener T, et al. Role of strengthening during nonoperative treatment of lateral epicondyle tendinopathy. J Hand Ther. 2021 Oct-Dec;34(4):619-26.
http://www.ncbi.nlm.nih.gov/pubmed/33250396?tool=bestpractice.com
Radial nerve mobilisation techniques have also been found to provide effective short-term pain relief in a small randomised controlled trial (RCT).[69]Yilmaz K, Yigiter Bayramlar K, Ayhan C, et al. Investigating the effects of neuromobilization in lateral epicondylitis. J Hand Ther. 2022 Jan-Mar;35(1):97-106.
http://www.ncbi.nlm.nih.gov/pubmed/33563509?tool=bestpractice.com
Patients should be monitored every 6-8 weeks for 6 months to assess progress, such as whether they have returned to work or are participating in any sport.
Other conservative measures
An overview of systematic reviews of the clinical effectiveness of conservative interventions suggested uncertainty as to the effectiveness of many conservative interventions for the treatment of lateral epicondylitis. This was mainly due to the small sample sizes in the RCTs that have been reported. Conclusions regarding cost-effectiveness were also unclear.[70]Long L, Briscoe S, Cooper C, et al. What is the clinical effectiveness and cost-effectiveness of conservative interventions for tendinopathy? An overview of systematic reviews of clinical effectiveness and systematic review of economic evaluations. Health Technol Assess. 2015 Jan;19(8):1-134.
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0082113/pdf/PubMedHealth_PMH0082113.pdf
http://www.ncbi.nlm.nih.gov/pubmed/25629427?tool=bestpractice.com
A meta-analysis of pooled data from RCTs indicated a lack of intermediate- to long-term clinical benefit after non-surgical treatment of lateral epicondylitis compared with observation only or placebo. Non-surgical treatments included injections (corticosteroid, platelet-rich plasma, autologous blood, sodium hyaluronate, or glycosaminoglycan polysulfate), physiotherapy, shock wave therapy, laser, ultrasound, corticosteroid iontophoresis, topical glyceryl trinitrate, or naproxen.[71]Sayegh ET, Strauch RJ. Does nonsurgical treatment improve longitudinal outcomes of lateral epicondylitis over no treatment? A meta-analysis. Clin Orthop Relat Res. 2015 Mar;473(3):1093-107.
https://link.springer.com/article/10.1007/s11999-014-4022-y/fulltext.html
http://www.ncbi.nlm.nih.gov/pubmed/25352261?tool=bestpractice.com
While corticosteroid injections have been shown to improve short-term pain relief (4-6 weeks) compared with both placebo and bracing, there is evidence that the long-term outcome following corticosteroid injection for treatment of tennis elbow is worse than no treatment or physiotherapy alone.[72]Gaujoux-Viala C, Dougados M, Gossec L. Efficacy and safety of steroid injections for shoulder and elbow tendonitis: a meta-analysis of randomised controlled trials. Ann Rheum Dis. 2009 Dec;68(12):1843-9.
http://ard.bmj.com/content/68/12/1843.long
http://www.ncbi.nlm.nih.gov/pubmed/19054817?tool=bestpractice.com
[73]Bisset L, Beller E, Jull G, et al. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ. 2006 Nov 4;333(7575):939.
http://www.bmj.com/content/333/7575/939
http://www.ncbi.nlm.nih.gov/pubmed/17012266?tool=bestpractice.com
One randomised controlled trial found that the use of corticosteroid injection versus placebo injection resulted in worse clinical outcomes after one year.[74]Coombes BK, Bisset L, Brooks P, et al. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial. JAMA. 2013 Feb 6;309(5):461-9.
http://jama.jamanetwork.com/article.aspx?articleid=1568252
http://www.ncbi.nlm.nih.gov/pubmed/23385272?tool=bestpractice.com
If a decision is reached to administer corticosteroid injections, care must be taken to avoid both the nerve medially (paralysis) and subcuticular adipose tissue (necrosis).[24]Ciccotti MG, Ramani MN. Medial epicondylitis. Tech Hand Up Extrem Surg. 2003 Dec;7(4):190-6.
http://www.ncbi.nlm.nih.gov/pubmed/16518220?tool=bestpractice.com
[37]Smidt N, Assendelft WJ, van der Windt DA, et al. Corticosteroid injections for lateral epicondylitis: a systematic review. Pain. 2002 Mar;96(1-2):23-40.
http://www.ncbi.nlm.nih.gov/pubmed/11932058?tool=bestpractice.com
[57]Johnson GW, Cadwallader K, Scheffel SB, et al. Treatment of lateral epicondylitis. Am Fam Physician. 2007 Sep 15;76(6):843-8.
http://www.ncbi.nlm.nih.gov/pubmed/17910298?tool=bestpractice.com
[72]Gaujoux-Viala C, Dougados M, Gossec L. Efficacy and safety of steroid injections for shoulder and elbow tendonitis: a meta-analysis of randomised controlled trials. Ann Rheum Dis. 2009 Dec;68(12):1843-9.
http://ard.bmj.com/content/68/12/1843.long
http://www.ncbi.nlm.nih.gov/pubmed/19054817?tool=bestpractice.com
[75]Barr S, Cerisola FL, Blanchard V. Effectiveness of corticosteroid injections compared with physiotherapeutic interventions for lateral epicondylitis: a systematic review. Physiotherapy. 2009 Dec;95(4):251-65.
http://www.ncbi.nlm.nih.gov/pubmed/19892089?tool=bestpractice.com
[76]Coombes BK, Bisset L, Vicenzino B, et al. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet. 2010 Nov 20;376(9754):1751-67.
http://www.ncbi.nlm.nih.gov/pubmed/20970844?tool=bestpractice.com
Refractory to treatment 6-12 months after initial presentation
Patients with epicondylitis who do not improve with the initial therapeutic interventions are referred to an orthopaedic consultant. Another thorough history and physical examination should be performed.
If recalcitrant epicondylitis is diagnosed (pain has persisted for 6-12 months after initial or recurrent presentation), surgical interventions will be considered. The use of injections with autologous blood/platelet-rich plasma, or extracorporeal shock wave therapy (ESWT), may be considered as alternative treatments to surgical intervention, but the evidence for these therapies is currently limited.
[  ]
How do platelet-rich therapies affect outcomes in people with musculoskeletal soft tissue injuries?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.680/fullShow me the answer
]
How do platelet-rich therapies affect outcomes in people with musculoskeletal soft tissue injuries?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.680/fullShow me the answer
Surgical interventions
Surgical intervention for both medial and lateral epicondylitis is limited to recalcitrant cases.[4]Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994 Jan;2(1):1-8.
http://www.ncbi.nlm.nih.gov/pubmed/10708988?tool=bestpractice.com
[24]Ciccotti MG, Ramani MN. Medial epicondylitis. Tech Hand Up Extrem Surg. 2003 Dec;7(4):190-6.
http://www.ncbi.nlm.nih.gov/pubmed/16518220?tool=bestpractice.com
[57]Johnson GW, Cadwallader K, Scheffel SB, et al. Treatment of lateral epicondylitis. Am Fam Physician. 2007 Sep 15;76(6):843-8.
http://www.ncbi.nlm.nih.gov/pubmed/17910298?tool=bestpractice.com
All patients should be informed pre-operatively of possible decreased grip strength after surgery.[4]Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994 Jan;2(1):1-8.
http://www.ncbi.nlm.nih.gov/pubmed/10708988?tool=bestpractice.com
Lateral epicondylitis
Systematic reviews have suggested that the current evidence is insufficient to support or refute the effectiveness of surgical intervention.[77]Buchbinder R, Johnston RV, Barnsley L, et al. Surgery for lateral elbow pain. Cochrane Database Syst Rev. 2011;(3):CD003525.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003525.pub2/full
http://www.ncbi.nlm.nih.gov/pubmed/21412883?tool=bestpractice.com
[78]Bateman M, Littlewood C, Rawson B, et al. Surgery for tennis elbow: a systematic review. Shoulder Elbow. 2019 Feb;11(1):35-44.
https://www.doi.org/10.1177/1758573217745041
http://www.ncbi.nlm.nih.gov/pubmed/30719096?tool=bestpractice.com
Systematic reviews and one randomised controlled trial (published subsequent to systematic review searches) report no significant differences between arthroscopic and open surgery (e.g., functional outcomes, failure rate, pain relief) in patients with lateral epicondylitis.[79]Moradi A, Pasdar P, Mehrad-Majd H, et al. Clinical Outcomes of Open versus Arthroscopic Surgery for Lateral Epicondylitis, Evidence from a Systematic Review. Arch Bone Jt Surg. 2019 Mar;7(2):91-104.
http://www.ncbi.nlm.nih.gov/pubmed/31211187?tool=bestpractice.com
[80]Wang W, Chen J, Lou J, et al. Comparison of arthroscopic debridement and open debridement in the management of lateral epicondylitis: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Nov;98(44):e17668.
https://www.doi.org/10.1097/MD.0000000000017668
http://www.ncbi.nlm.nih.gov/pubmed/31689781?tool=bestpractice.com
[81]Clark T, McRae S, Leiter J, et al. Arthroscopic Versus Open Lateral Release for the Treatment of Lateral Epicondylitis: A Prospective Randomized Controlled Trial. Arthroscopy. 2018 Dec;34(12):3177-3184.
https://www.doi.org/10.1016/j.arthro.2018.07.008
http://www.ncbi.nlm.nih.gov/pubmed/30509427?tool=bestpractice.com
One review found that post-operative complications (such as mild flexion-extension limitation, haematoma, wound infection, revision requirement, forearm paresthesias for 2 weeks after surgery) were significantly more common following open surgery.[79]Moradi A, Pasdar P, Mehrad-Majd H, et al. Clinical Outcomes of Open versus Arthroscopic Surgery for Lateral Epicondylitis, Evidence from a Systematic Review. Arch Bone Jt Surg. 2019 Mar;7(2):91-104.
http://www.ncbi.nlm.nih.gov/pubmed/31211187?tool=bestpractice.com
Arthroscopic surgery was associated with increased operative time.[80]Wang W, Chen J, Lou J, et al. Comparison of arthroscopic debridement and open debridement in the management of lateral epicondylitis: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Nov;98(44):e17668.
https://www.doi.org/10.1097/MD.0000000000017668
http://www.ncbi.nlm.nih.gov/pubmed/31689781?tool=bestpractice.com
[81]Clark T, McRae S, Leiter J, et al. Arthroscopic Versus Open Lateral Release for the Treatment of Lateral Epicondylitis: A Prospective Randomized Controlled Trial. Arthroscopy. 2018 Dec;34(12):3177-3184.
https://www.doi.org/10.1016/j.arthro.2018.07.008
http://www.ncbi.nlm.nih.gov/pubmed/30509427?tool=bestpractice.com
Long-term follow up data are limited. Single-surgeon series (with mean follow-up >9.8 years) report subjective overall improvement in >90% of patients who underwent an open surgical procedure for lateral epicondylitis.[82]Dunn JH, Kim JJ, Davis L, et al. Ten- to 14-year follow-up of the Nirschl surgical technique for lateral epicondylitis. Am J Sports Med. 2008 Feb;36(2):261-6.
http://www.ncbi.nlm.nih.gov/pubmed/18055917?tool=bestpractice.com
[83]Coleman B, Quinlan JF, Matheson JA. Surgical treatment for lateral epicondylitis: a long-term follow-up of results. J Shoulder Elbow Surg. 2010 Apr;19(3):363-7.
https://www.doi.org/10.1016/j.jse.2009.09.008
http://www.ncbi.nlm.nih.gov/pubmed/20004594?tool=bestpractice.com
In one series, patient satisfaction averaged 8.9/10.[82]Dunn JH, Kim JJ, Davis L, et al. Ten- to 14-year follow-up of the Nirschl surgical technique for lateral epicondylitis. Am J Sports Med. 2008 Feb;36(2):261-6.
http://www.ncbi.nlm.nih.gov/pubmed/18055917?tool=bestpractice.com
Medial epicondylitis
Surgical intervention for medial epicondylitis involves the open debridement and excision of the undersurface of the flexor pronator mass. Mean subjective estimate of elbow function has been found to improve from 38% to 98% of normal after surgery for medial epicondylitis.[84]Vangsness CT Jr, Jobe FW. Surgical treatment of medial epicondylitis: results in 35 elbows. J Bone Joint Surg Br. 1991 May;73(3):409-11.
http://www.bjj.boneandjoint.org.uk/content/jbjsbr/73-B/3/409.full.pdf
http://www.ncbi.nlm.nih.gov/pubmed/1670439?tool=bestpractice.com
Possible adverse effects of surgery include injury to the ulnar nerve and/or weakness with wrist flexion.[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: probe placed on area of degenerative tendon showing loss of normal tendon appearanceFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: pick-ups lifting off area of degenerative tendon after elliptical incision to excise this areaFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: pick-ups lifting off area of degenerative tendon after elliptical incision to excise this areaFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].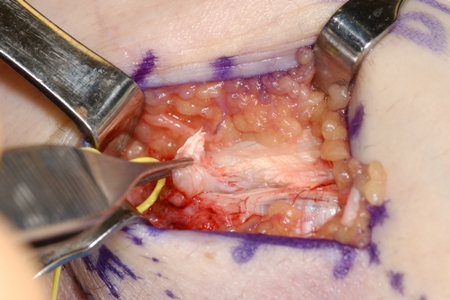 [Figure caption and citation for the preceding image starts]: Markings for swing incision location for patient with chronic refractory medial epicondylitisFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Markings for swing incision location for patient with chronic refractory medial epicondylitisFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].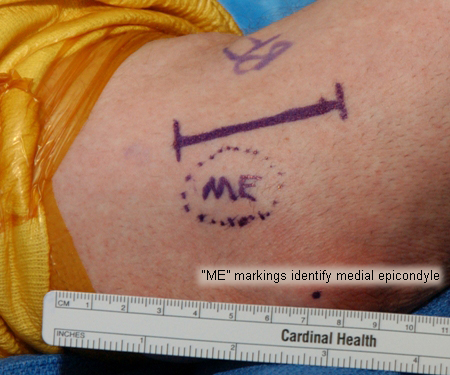 [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: degenerative tendon removedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: degenerative tendon removedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: medial epicondyle exposedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Surgery for refractory medial epicondylitis: medial epicondyle exposedFrom the collection of Dr Brian Fitzgerald, Naval Medical Center San Diego, CA; used with permission [Citation ends].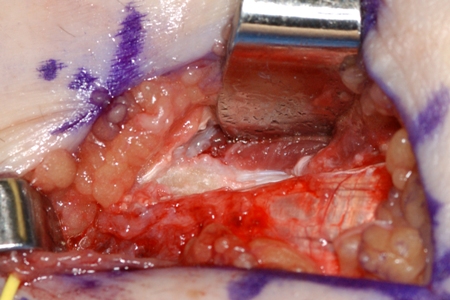
Ultrasound-guided minimally invasive tenotomy
Ultrasound-guided minimally invasive tenotomy has shown symptomatic improvement in non-randomised studies.[85]Dakkak M, Patel V, King D, et al. Ultrasound-guided tenotomy for lateral epicondylitis with TenJet improves physical functional and decreased pain outcomes at 1 year: a case series review. JSES Int. 2023 Sep;7(5):872-6.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10499850
http://www.ncbi.nlm.nih.gov/pubmed/37719823?tool=bestpractice.com
It is a safe and effective treatment option for chronic refractory lateral and medial elbow tendinopathy, showing significant pain and function improvements over one year. Further research is required to assess its effectiveness in diverse patient populations using controlled study designs.[86]Barnes DE, Beckley JM, Smith J. Percutaneous ultrasonic tenotomy for chronic elbow tendinosis: a prospective study. J Shoulder Elbow Surg. 2015 Jan;24(1):67-73.
http://www.ncbi.nlm.nih.gov/pubmed/25306494?tool=bestpractice.com
Dry needling
Dry needling is a low-cost, minimally invasive, and low-risk therapy for refractory lateral epicondylitis. It involves multiple needle insertions into the extensor carpi radialis brevis tendon and is usually performed percutaneously under local anaesthetic. Dry needling has been shown to provide symptomatic improvement in a few small studies.[87]Uygur E, Aktaş B, Özkut A, et al. Dry needling in lateral epicondylitis: a prospective controlled study. Int Orthop. 2017 Nov;41(11):2321-5.
http://www.ncbi.nlm.nih.gov/pubmed/28828509?tool=bestpractice.com
[88]Nagarajan V, Ethiraj P, Prasad P A, et al. Local corticosteroid injection versus dry needling in the treatment of lateral epicondylitis. Cureus. 2022 Nov;14(11):e31286.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9733488
http://www.ncbi.nlm.nih.gov/pubmed/36514597?tool=bestpractice.com
Extracorporeal shock wave therapy
Extracorporeal shock wave therapy (ESWT) may be effective in patients desiring to avoid surgery or in people with risk factors precluding surgery.[89]Kohia M, Brackle J, Byrd K, et al. Effectiveness of physical therapy treatments on lateral epicondylitis. J Sport Rehabil. 2008 May;17(2):119-36.
http://www.ncbi.nlm.nih.gov/pubmed/18515912?tool=bestpractice.com
ESWT is not indicated in cases of medial epicondylitis. Systematic reviews suggest that extracorporeal shock wave therapy may be of modest benefit in the management of lateral epicondylitis, but high-quality RCTs are required.[90]Xiong Y, Xue H, Zhou W, et al. Shock-wave therapy versus corticosteroid injection on lateral epicondylitis: a meta-analysis of randomized controlled trials. Phys Sportsmed. 2019 Sep;47(3):284-289.
https://www.doi.org/10.1080/00913847.2019.1599587
http://www.ncbi.nlm.nih.gov/pubmed/30951399?tool=bestpractice.com
[91]Yao G, Chen J, Duan Y, et al. Efficacy of Extracorporeal Shock Wave Therapy for Lateral Epicondylitis: A Systematic Review and Meta-Analysis. Biomed Res Int. 2020;2020:2064781.
https://www.doi.org/10.1155/2020/2064781
http://www.ncbi.nlm.nih.gov/pubmed/32309425?tool=bestpractice.com
Injection therapy
Injection modalities, including autologous blood, platelet-rich plasma, hyaluronic acid, and botulinum toxin, have been proposed as treatments for recalcitrant lateral and medial epicondylitis.
Autologous blood or platelet-rich plasma
Injected into the tendons for medial and lateral epicondylitis and is thought to stimulate a local inflammatory response.
The use of injections with autologous blood/platelet-rich plasma, or extracorporeal shock wave therapy (ESWT), may be considered as alternate treatments to surgical intervention, but the evidence for these therapies is currently limited.[92]Ahmad Z, Brooks R, Kang SN, et al. The effect of platelet-rich plasma on clinical outcomes in lateral epicondylitis. Arthroscopy. 2013 Nov;29(11):1851-62.
http://www.ncbi.nlm.nih.gov/pubmed/24060428?tool=bestpractice.com
[93]Krogh TP, Bartels EM, Ellingsen T, et al. Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review and network meta-analysis of randomized controlled trials. Am J Sports Med. 2013 Jun;41(6):1435-46.
http://www.ncbi.nlm.nih.gov/pubmed/22972856?tool=bestpractice.com
The National Institute for Health and Care Excellence (NICE) recommends autologous blood products for the treatment of tendinopathy; however, their effectiveness is uncertain.[94]National Institute for Health and Care Excellence. Autologous blood injection for tendinopathy. Jan 2013 [internet publication].
https://www.nice.org.uk/guidance/ipg438
Two systematic reviews in patients with lateral epicondylitis reported that autologous blood or platelet-rich plasma significantly improved pain and elbow function in the intermediate term (12-26 weeks), and that platelet-rich plasma injection improved function and pain at 24 weeks, compared with corticosteroid injections.[95]Houck DA, Kraeutler MJ, Thornton LB, et al. Treatment of Lateral Epicondylitis With Autologous Blood, Platelet-Rich Plasma, or Corticosteroid Injections: A Systematic Review of Overlapping Meta-analyses. Orthop J Sports Med. 2019 Mar;7(3):2325967119831052.
https://www.doi.org/10.1177/2325967119831052
http://www.ncbi.nlm.nih.gov/pubmed/30899764?tool=bestpractice.com
[96]Li A, Wang H, Yu Z, et al. Platelet-rich plasma vs corticosteroids for elbow epicondylitis: A systematic review and meta-analysis. Medicine (Baltimore). 2019 Dec;98(51):e18358.
https://www.doi.org/10.1097/MD.0000000000018358
http://www.ncbi.nlm.nih.gov/pubmed/31860992?tool=bestpractice.com
However, a subsequent Cochrane review concluded that autologous blood/platelet-rich plasma injections provide little or no clinically important benefit for pain or function in patients with lateral elbow pain.[97]Karjalainen TV, Silagy M, O'Bryan E, et al. Autologous blood and platelet-rich plasma injection therapy for lateral elbow pain. Cochrane Database Syst Rev. 2021 Sep 30;9:CD010951.
http://www.ncbi.nlm.nih.gov/pubmed/34590307?tool=bestpractice.com
It also reported that it is uncertain whether the injections improve treatment success or pain relief (>50%).[97]Karjalainen TV, Silagy M, O'Bryan E, et al. Autologous blood and platelet-rich plasma injection therapy for lateral elbow pain. Cochrane Database Syst Rev. 2021 Sep 30;9:CD010951.
http://www.ncbi.nlm.nih.gov/pubmed/34590307?tool=bestpractice.com
[ ]
How do platelet-rich therapies affect outcomes in people with musculoskeletal soft tissue injuries?/cca.html?targetUrl=https://cochranelibrary.com/cca/doi/10.1002/cca.680/fullShow me the answer
Botulinum toxin
Reduced pain following botulinum toxin injection has been reported in people with lateral epicondylitis, but there is also a high risk of complications, including digital paresis and weakness.[98]Wong SM, Hui AC, Tong PY, et al. Treatment of lateral epicondylitis with botulinum toxin: a randomized, double-blind, placebo-controlled trial. Ann Intern Med. 2005 Dec 6;143(11):793-7.
http://www.ncbi.nlm.nih.gov/pubmed/16330790?tool=bestpractice.com
[99]Kalichman LB, Bannuru RR, Severin M, et al. Injection of botulinum toxin for treatment of chronic lateral epicondylitis: systematic review and meta-analysis. Sem Arthritis Rheum. 2011 Jun;40(6):532-8.
http://www.ncbi.nlm.nih.gov/pubmed/20822798?tool=bestpractice.com
[100]Zhang T, Adatia A, Zarin W, et al. The efficacy of botulinum toxin type A in managing chronic musculoskeletal pain: a systematic review and meta analysis. Inflammopharmacology. 2011 Feb;19(1):21-34.
http://www.ncbi.nlm.nih.gov/pubmed/21076878?tool=bestpractice.com
[101]Lin YC, Wu WT, Hsu YC, et al. Comparative effectiveness of botulinum toxin versus non-surgical treatments for treating lateral epicondylitis: a systematic review and meta-analysis. Clin Rehabil. 2018 Feb;32(2):131-145.
https://www.doi.org/10.1177/0269215517702517
http://www.ncbi.nlm.nih.gov/pubmed/28349703?tool=bestpractice.com
Hyaluronic acid
Hyaluronic acid injections have been shown to improve pain and grip strength in patients with chronic lateral epicondylitis when compared with placebo. No serious adverse effects were reported and improvement persisted after 1 year.[102]Petrella RJ, Cogliano A, Decaria J, et al. Management of tennis elbow with sodium hyaluronate periarticular injections. Sports Med Arthrosc Rehabilit Ther Technol. 2010 Feb 2;2:4.
http://www.biomedcentral.com/1758-2555/2/4
http://www.ncbi.nlm.nih.gov/pubmed/20205851?tool=bestpractice.com
However, few high-quality studies are available.
Low-level laser therapy
Optimally dosed low-level laser therapy administered directly to the lateral elbow tendon insertions may offer short-term pain relief and less disability in lateral epicondylitis, both alone and in conjunction with an exercise regimen. There is conflicting evidence for the efficacy of this intervention.[103]Bjordal JM, Lopes-Martins RA, Joensen J, et al. A systematic review with procedural assessments and meta-analysis of low level laser therapy in lateral elbow tendinopathy (tennis elbow). BMC Musculoskelet Disord. 2008 May 29;9:75.
http://www.biomedcentral.com/1471-2474/9/75
http://www.ncbi.nlm.nih.gov/pubmed/18510742?tool=bestpractice.com
[104]Baxter GD, Bleakley C, McDonough S. Clinical effectiveness of laser acupuncture: a systematic review. J Acupunct Meridian Stud. 2008 Dec;1(2):65-82.
http://www.jams-kpi.com/article/S2005-2901(09)60026-1/fulltext
http://www.ncbi.nlm.nih.gov/pubmed/20633458?tool=bestpractice.com
[105]Chang WD, Wu JH, Yang WJ, et al. Therapeutic effects of low-level laser on lateral epicondylitis from differential interventions of Chinese-Western medicine: systematic review. Photomed Laser Surg. 2010 Jun;28(3):327-36.
http://www.ncbi.nlm.nih.gov/pubmed/19874256?tool=bestpractice.com
[106]Tumilty S, Munn J, McDonough S, et al. Low level laser treatment of tendinopathy: a systematic review with meta-analysis. Photomed Laser Surg. 2010 Feb;28(1):3-16.
http://www.ncbi.nlm.nih.gov/pubmed/19708800?tool=bestpractice.com
[107]Roberts DB, Kruse RJ, Stoll SF. The effectiveness of therapeutic class IV (10 W) laser treatment for epicondylitis. Lasers Surg Med. 2013 Jul;45(5):311-7.
http://www.ncbi.nlm.nih.gov/pubmed/23733499?tool=bestpractice.com