Investigations
1st investigations to order
upper gastrointestinal contrast series
Test
Only indicated if the patient appears stable and does not require immediate surgery for suspected volvulus. Diagnostic standard test for malrotation, and should be performed with anteroposterior (AP) and lateral projections if there is any history of bilious vomiting without previous abdominal surgery.[12][13]
Normal pattern of rotation: the transition of duodenum to jejunum (ligament of Treitz) lying left of the left vertebral pedicles in AP view. The position of this transition should also be at the level of the pylorus or superior to this.[Figure caption and citation for the preceding image starts]: Malrotation with volvulus without obstruction as seen on upper GI contrastFrom the collection of Dr S.D. St Peter [Citation ends].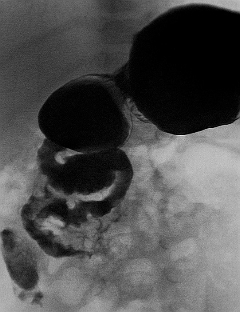
Normal anatomy on this examination rules out malrotation, midgut volvulus, and obstruction of the upper small intestine.
The typical sensitivity is approximately 95%, but it may have a false-positive rate of up to 15% and false-negative rate of up to 6%.[13][14][15]
Delayed images in 1 or 2 hours can depict or rule out obstruction of the distal small bowel.
Result
right-sided duodenum (malrotation); duodenum courses inferior or medial to normal (malrotation); bird-beak cut-off of duodenum (volvulus); corkscrew of duodenum (volvulus); a web in the duodenum (duodenal atresia)
abdominal plain x-rays
Test
Usually ordered in the accident and emergency department for patients presenting with abdominal complaints, but is rarely helpful in changing management or preventing other tests.
In the newborn nursery, a patient with bilious vomiting is typically studied first with emergency plain films, as they provide a better yield for demonstrating other congenital aetiologies for symptoms.[12]
Stomach and proximal duodenum distended with gas and some distal gas is the most consistent but non-specific sign of volvulus on plain films.[16]
The build-up of air in the stomach and proximal duodenum during volvulus may give the double-bubble appearance that is otherwise pathognomonic for duodenal atresia, but if any air is present distally, malrotation with volvulus is suggested and an emergency upper gastrointestinal (GI) series should be performed (assuming the patient does not require immediate surgery).
If the amount of distended loops of bowel is large, this is suggestive more of a distal bowel obstruction, but a midgut volvulus cannot be ruled out. A carefully combined upper and lower GI series may need to be performed in co-ordination with the paediatric radiologist.
A normal abdominal radiograph does not exclude the diagnosis of malrotation.[12]
Result
distended stomach and proximal duodenum with paucity of bowel gas seen distally (volvulus or duodenal web); normal x-ray (malrotation without volvulus or volvulus without complete obstruction)
Investigations to consider
ultrasound
Test
Can be done quickly without contrast or radiation, but if midgut volvulus is a concern, it may be clinically misguided to order an ultrasound.[12]
An ultrasound is more commonly ordered to assess for intussusception if malrotation or midgut volvulus is not the primary consideration. However, when it is ordered to rule out intussusception, or in circumstances where the upper gastrointestinal series is not conclusive, images of the mesenteric vessels may be useful, demonstrating a reversed superior mesenteric artery-superior mesenteric artery and vein (SMA-SMV) relationship or even a "whirlpool" pattern of volvulus.[12] One meta-analysis and narrative review focussed on the role of ultrasound to diagnose, or exclude, malrotation/volvulus. A careful protocol with visualisation of the course of the duodenum, as well as the relationship of the SMA/SMV, may improve diagnostic accuracy for midgut malrotation in children.[18][19] The meta-analysis also reported a high summary sensitivity and specificity of 94% and 100% respectively, for the use of ultrasound in diagnosing malrotation with or without midgut volvulus.[19]
Result
no flow beyond the proximal SMA volvulus with ischaemia; twirling of the superior SMV volvulus. Caution is required if a normal SMA/SMV relationship is demonstrated or reported - this does not exclude malrotation
lower gastrointestinal (GI) contrast series
Test
May be ordered in the work-up of newborn patients with stooling difficulty or distal intestinal obstruction.[12]
Malrotation may be suspected by abnormal position of the caecum (present in 85%).[17]
If there is any concern of GI obstruction, the abnormal caecal position should prompt upper GI contrast study.
Rarely, lower GI series may augment the investigation for malrotation if the upper GI series is inconclusive.[17]
Result
abnormal position of the caecum
CT abdomen (with oral and intravenous contrast)
Test
Not the preferred study to assess for malrotation and/or midgut volvulus. May be considered when the presentation is abdominal pain without witnessed vomiting, and the concern for malrotation is low. If midgut volvulus is being considered, then CT scan should not be performed before an upper gastrointestinal (GI) series.[17]
Performed using oral and intravenous contrast to delineate intestinal pathologies.
Coronal reconstructions are particularly useful in following the course of the duodenum to assure the transition from duodenum to jejunum lies left of the left side of the spine and is appropriately high enough.
Additional information that can be obtained from the scan, which is not offered by the upper GI contrast series, is immediate assessment of caecal position/colonic rotation and 3-dimensional evaluation of the entire extra-intestinal space.
Result
no oral contrast beyond duodenum (volvulus); no contrast in the distal superior mesenteric artery (volvulus with ischaemia); twirling of the superior mesenteric artery and vein (volvulus); transposition of superior mesenteric artery and vein (malrotation); a transition point in bowel calibre, right-sided duodenum; duodenum courses anterior or to right of superior mesenteric artery
ABG (including lactate)
Test
When bowel perfusion is compromised from twisting of the mesenteric vessels, lactic acidosis ensues dropping the serum pH with increased anion gap.
Acidosis is non-specific and non-diagnostic. If the diagnosis of volvulus is confirmed with radiological studies, blood gas analysis is important to know the physiological status of the patient and to guide resuscitation.
Result
metabolic acidosis with respiratory alkalosis resulting in profound decrease in partial pressure of carbon dioxide. Raised lactate indicates poor tissue perfusion.
Clotting, group and save, or cross-match
Test
Required if surgery is being considered.[21]
Result
For operating theatre use.
Urea and electrolytes
Test
Patients with volvulus and resultant bowel ischaemia can develop severe metabolical derangements, which may require correction.
Result
Non-specific for diagnosis. Hypochloraemia and hypokalaemia can be associated with persistent obstruction associated with nausea and vomiting. May indicate degree of volume depletion that is secondary to the obstruction.
FBC
Use of this content is subject to our disclaimer