Investigations
1st investigations to order
chest x-ray
Test
Symptomatic patients should have this study because of its simplicity and relatively low cost.[1][Figure caption and citation for the preceding image starts]: Type IV para-oesophageal hiatus hernia: (A) Frontal chest x-ray revealing a large intrathoracic gastric bubble (arrows); (B) Air-fluid level confirming intrathoracic gastric contents on the right lateral decubitus chest x-ray (arrow)BMJ Case Reports 2009 (doi:10.1136/bcr.06.2008.0302); copyright@2009 by the BMJ Publishing Group [Citation ends].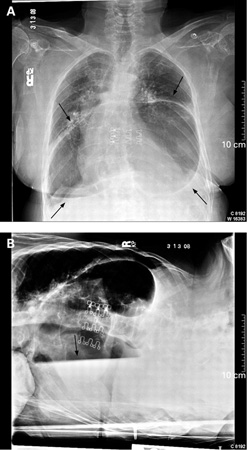
Result
retrocardiac air bubble or normal
upper gastrointestinal fluoroscopy with oral contrast
Test
This is the standard test; it will delineate the anatomy and provide a qualitative assessment of oesophageal motility.[17][18] Patients with moderate-to-severe symptoms from a suspected hiatus hernia should have this study.
Fluoroscopy may be performed with a barium oesophagram, but an upper gastrointestinal series evaluation is recommended if the hernia is large for a complete assessment of the stomach.[17]
Result
stomach is partially or completely intrathoracic
Investigations to consider
oesophago-gastro-duodenoscopy
Test
Patients with moderate-to-severe reflux symptoms should undergo endoscopy to check for the presence of oesophagitis or oesophageal dysplasia.[6] The findings are helpful in directing therapy.
Result
inflammation of the oesophagus and proximal migration of the gastro-oesophageal junction
CT scan or MRI scan
Test
CT or MRI imaging is indicated when the diagnosis is not clear, other pathology is suspected, or when planning surgical intervention.[1] These scans provide a 3-dimensional reconstruction of the anatomy and thus determine whether organs other than the stomach have migrated into the chest.
Result
may show partial or complete intrathoracic stomach and herniation of other intra-abdominal organs into the chest
high-resolution oesophageal manometry and pH monitoring
Test
Oesophageal manometry and pH monitoring are indicated in patients with hiatus hernia and atypical symptoms, dysphagia, and/or when additional confirmation of the diagnosis is required.[19] High resolution manometry (HRM) should be utilised as it can demonstrate various anatomical landmarks, such as the level of the diaphragmatic crura or the location of the lower oesophageal sphincter. Calculating the size of a sliding component of a hiatus hernia is also possible with HRM.[1]
Abnormal pH monitoring results are seen with larger hiatus hernias. While this is not a necessary investigation for the diagnosis of hiatus hernia, it is useful when evaluating the need for anti-reflux surgery in addition to hernia repair.[1][20]
Result
double hump configuration on manometry, normal or abnormal 24-hour pH
Use of this content is subject to our disclaimer