History and exam
Key diagnostic factors
common
presence of risk factors
Key risk factors include viral infections, acute or chronic otitis media, meningitis, cholesteatoma, and inner ear malformations.
vertigo
Patients typically describe 'room-spinning' (acute rotational) vertigo of peripheral origin.[13]
Vertigo is of gradual onset and develops over several hours; sustained vertigo may follow, which lasts from days to weeks. The vertigo in patients with labyrinthitis and vestibular neuritis may be present at rest unlike that in patients with benign paroxysmal positional vertigo. Nevertheless, it may be triggered by movements.[5]
dizziness
Can mean a variety of things, including floating, imbalance, disequilibrium, and impaired cognition.
nausea and vomiting
Nausea and vomiting may be of variable duration, typically lasting from several hours to days.[13]
hearing loss
Typical in labyrinthitis presentation. May be unilateral or bilateral.
Hearing is intact in vestibular neuritis as the cochlea is not affected.
nystagmus
tinnitus
Possible presentation (constant noise in the ear) in labyrinthitis. Uncommon in vestibular neuritis.[13]
otorrhoea
Ear discharge alerts to presence of acute or chronic otitis media with tympanic membrane perforation.
Other diagnostic factors
common
vertigo-related quick head or body movements
Follow acute vertigo; indicate incomplete vestibular compensation.
influenza-like symptoms
Viral labyrinthitis may occur during an influenza-like illness or during illnesses such as measles or mumps. Fever, sore throat, and influenza-like symptoms may be present if labyrinthitis or vestibular neuritis occur during an influenza-like illness or during illnesses such as measles or mumps.[16]
uncommon
otalgia
Pain in the ear may be present in patients with acute or chronic otitis media.
Risk factors
strong
viral infections
Viral infections are presumed to be the most common cause of labyrinthitis and vestibular neuritis due to the absence of other overt diagnostic causes such as the other entities listed in this section. Viral illnesses, in particular DNA viruses, have a known association with other mononeuropathies, such as Bell's palsy, optic neuritis, and peritoneal neuronitis.
Aetiological viral agents for labyrinthitis include varicella zoster virus, cytomegalovirus, mumps virus, measles virus, rubella virus, and HIV, and those for vestibular neuritis include influenza virus, adenovirus, herpes simplex virus, cytomegalovirus, Epstein-Barr virus, rubella virus, and parainfluenza virus.[3][16][18]
chronic suppurative otitis media
Chronic middle ear infections such as chronic suppurative otitis media (CSOM, a persistent inflammation of the middle ear or mastoid cavity), if not treated in a timely manner, may lead to diffusion of bacterial toxins into the inner ear.[30]
Direct bacterial invasion into the otic capsule has been demonstrated in CSOM with or without accompanying cholesteatoma.
acute otitis media
Acute infections of the middle ear most typically result in serous labyrinthitis secondary to diffusion of bacterial toxins into the membranous labyrinth.[2][30] Bacterial invasion into the inner ear does not occur in this setting, rather, toxins from the bacteria in the middle ear diffuse into the inner ear causing a serous labyrinthitis picture.
cholesteatoma
Direct erosion into the labyrinth or internal auditory canal by cholesteatoma (a collection of epidermal and connective tissues within the middle ear) increases the risk of developing labyrinthitis.[30]
[Figure caption and citation for the preceding image starts]: An axial CT (without contrast) of the temporal bone of the left ear demonstrating direct erosion into the horizontal semicircular canal by cholesteatomaFrom the personal collection of Dr Tiffany Hwa; used with permission [Citation ends].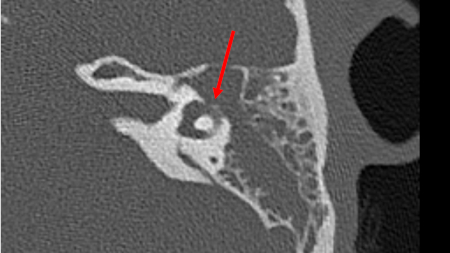
meningitis
Serous labyrinthitis results from bacterial toxins diffusing through the round window or internal auditory canal. Bacterial meningitis may result in labyrinthitis via spread of infection and inflammatory mediators into the inner ear via the cochlear aqueduct. The cochlear aqueduct connects the subarachnoid space to the scala tympani of the proximal basal turn of the cochlea. Meningitis secondary to Streptococcus pneumoniae poses the greatest risk for labyrinthitis and resultant hearing loss.[31]
inner ear malformations
Commonly associated with abnormal communications between the inner and middle ear.
weak
autoimmune ear diseases
Labyrinthitis has been associated with autoimmune inner ear disease (e.g., Cogan's syndrome or Behcet's disease). These rare diseases cause immune-mediated inner ear damage with resultant hearing loss and vestibular dysfunction.
syphilis
History of sexually transmitted disease increases risk of having contracted syphilis.[3] If left untreated, syphilis may eventually affect the central nervous system and the inner ear (tertiary neurosyphilis).
Use of this content is subject to our disclaimer