History and exam
Key diagnostic factors
common
presence of risk factors
Key factors include inadequate exposure to sunlight, age <18 months, breastfeeding, inadequate calcium and phosphate intake, and positive family history.
Other diagnostic factors
common
bone pain
May be associated with pseudofractures or insufficiency fractures.[3]
growth faltering
Faltering growth is a common presentation of rickets.[4]
delayed achievement of motor milestones
Consider rickets in children presenting with developmental delay.[4]
bony deformities
Such as bowlegs.[4][Figure caption and citation for the preceding image starts]: Malnutrition manifested as rickets. Note the bowed legs and kneesCDC [Citation ends].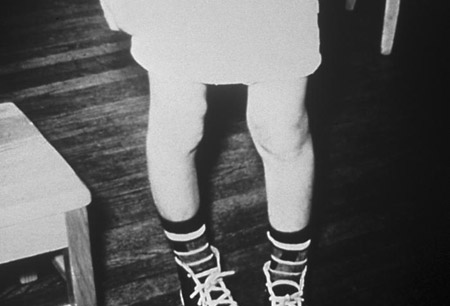
muscle weakness
May be due to hypocalcaemia or hypophosphataemia.[4]
uncommon
carpopedal spasm
May be seen associated with hypocalcaemia.
numbness or paresthesias
May be seen in association with hypocalcaemia.
tetany
May be seen associated with hypocalcaemia.
hypocalcaemic seizures
Can be a manifestation of rickets associated with hypocalcaemia.[4]
Risk factors
strong
age 6 to 23 months
inadequate sunlight exposure
breastfeeding
Breast milk is deficient in vitamin D. Without nutritional supplementation, rickets is possible.[3]
calcium deficiency
Inadequate intake of calcium can lead to insufficient bone mineralisation. Breast milk contains limited amounts of calcium, but cows' milk is a richer source.[4] In societies without a tradition of milk-drinking, calcium intake is often <300 mg daily. The net absorption of calcium and other minerals is limited by other food substances such as phytate, present in most cereals.[3]
phosphate deficiency
Inadequate intake of phosphorus can lead to insufficient bone mineralisation. Phosphorus is abundant in most diets but may not be sufficient in rapidly growing low-birth-weight babies. Phosphate may be precipitated in the stomach by antacids.[3]
family history of rickets
A family history of short stature, orthopaedic abnormalities, poor dentition, alopecia, and parental consanguinity may signify inherited rickets.[4]
antacids, loop diuretics, corticosteroids, or anticonvulsants
weak
darker skin complexion
Increased skin pigmentation may require increased exposure to sunlight to allow adequate conversion of 7-dehydrocholesterol to colecalciferol.[3]
Use of this content is subject to our disclaimer