Treatment algorithm
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups: see disclaimer
stretching exercises
The subacute phase is characterised by subsiding inflammation and pain. During this phase, emphasis is on stretching of the iliotibial band and soft-tissue therapy for any myofascial restrictions (e.g., trigger points, muscle contractures, fascial adhesions) which supports muscle strengthening and re-education.[Figure caption and citation for the preceding image starts]: Standing stretch exerciseFrom the personal collection of Dr J.C. Mak [Citation ends].
foam roll mobilisation
Treatment recommended for ALL patients in selected patient group
Foam roll mobilisation can be combined with stretching exercises to improve myofascial restrictions along the lateral hip and thigh.[41][Figure caption and citation for the preceding image starts]: Foam roll exerciseFrom the personal collection of Dr J.C. Mak [Citation ends].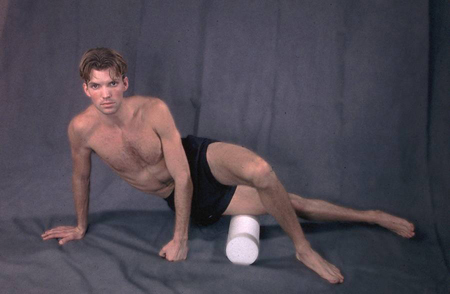
recovery and strengthening
Treatment recommended for ALL patients in selected patient group
Once range-of-motion and myofascial restrictions have been resolved with stretching exercises and foam roll mobilisation, recovery and strengthening can begin with exercises to promote movement patterns and improve hip abductor strength.
Electromyography studies suggest that contractions above 60% of the maximal voluntary isometric contraction are needed for strengthening.[42][43] This intensity is achieved with progression into single leg squat exercises and use of resistance (e.g., 2.3 kg [5 lb] ankle weight with side-lying hip abduction).[42][Figure caption and citation for the preceding image starts]: Demonstration of pelvic dropFrom the personal collection of Dr J.C. Mak [Citation ends].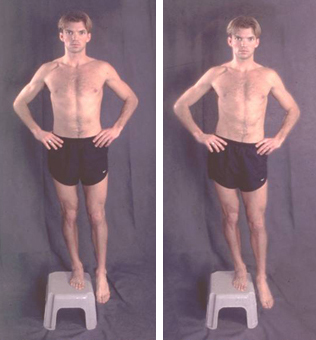
Choose a patient group to see our recommendations
Please note that formulations/routes and doses may differ between drug names and brands, drug formularies, or locations. Treatment recommendations are specific to patient groups. See disclaimer
Use of this content is subject to our disclaimer