History and exam
Key diagnostic factors
common
presence of risk factors
corona phlebectatica (malleolar flare or ankle flare)
ankle swelling
Usually unilateral but may be bilateral. Swelling due to oedema is common. It characteristically indents with pressure and initially occurs in the ankle region but may extend to the leg and foot.[2][10][Figure caption and citation for the preceding image starts]: Serial images of severe CVI (C6) and chronic ulceration of the right lower extremityFrom the collection of Dr Joseph L. Mills; used with permission [Citation ends].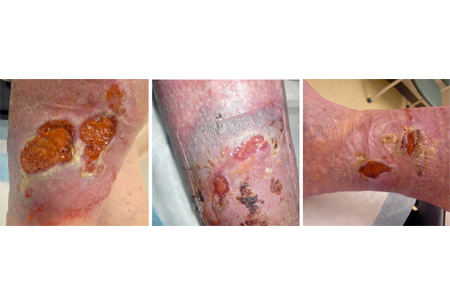
hyperpigmentation (brawny oedema)
Reddish-brown discoloration affecting the ankle and lower leg. Common in advanced disease. Results from extravasation of blood and deposition of haemosiderin in the tissues due to long-standing ambulatory venous hypertension.[2][10][Figure caption and citation for the preceding image starts]: Lipodermatosclerosis and leg ulcer with hypercoagulable state and recurrent episodes of deep vein thrombosis (DVT)From the collection of Dr Joseph L. Mills; used with permission [Citation ends].
lipodermatosclerosis
Localised chronic inflammatory and fibrotic condition affecting the skin and subcutaneous tissues of the lower leg, especially in the supramalleolar region. Common in advanced disease. When severe it may even lead to contracture of the Achilles tendon. Results from capillary proliferation, fat necrosis, and fibrosis of the skin and subcutaneous tissues.[2][10][Figure caption and citation for the preceding image starts]: Lipodermatosclerosis and leg ulcer with hypercoagulable state and recurrent episodes of deep vein thrombosis (DVT)From the collection of Dr Joseph L. Mills; used with permission [Citation ends].
atrophie blanche
Localised, frequently round areas of white, shiny, atrophic skin surrounded by small dilated capillaries and sometimes areas of hyperpigmentation. Common in advanced disease.[2][10][Figure caption and citation for the preceding image starts]: Atrophie blanche in a patient with CVIFrom the collection of Dr Joseph L. Mills; used with permission [Citation ends].
leg ulcers
Venous ulcers are located in the gaiter area (between the malleolus and mid-calf) of the calf, proximal and posterior to the medial malleolus, and occasionally superior to the lateral malleolus.[2][10]
Ulceration may be healed or active. [Figure caption and citation for the preceding image starts]: Serial images of recurrent venous ulcer with resolution at 3 monthsFrom the collection of Dr Joseph L. Mills; used with permission [Citation ends].
Other diagnostic factors
common
leg fatigue, aching, and/or discomfort
heavy legs
telangiectasias
reticular veins
dry and scaly skin
Eczematous skin changes are typical of venous stasis dermatitis.[10]
uncommon
Risk factors
strong
increasing age
Prevalence of venous disease increases with age.[11]
family history
Strong risk factor for acute and chronic venous disease.[11]
smoking
Cigarette smoking is an independent risk factor for severe CVI in men.[11]
deep vein thrombosis
As many as 50% of people develop CVI within 5-10 years of an episode of deep vein thrombosis (DVT) due to increased dilation of the venous system leading to axial system reflux.
orthostatic occupation
Occupations (e.g., builder) that require prolonged standing are thought to predispose to venous insufficiency.[11]
weak
female sex
Leg injury, prolonged standing, increasing parity, and cardiovascular disease are all strongly associated with venous insufficiency in women.[11]
obesity (waist circumference)
Increased body mass index (BMI) and waist circumference increase the risk of chronic venous disease.[11]
ligamentous laxity
Risk of CVI is increased in those with ligamentous laxity, suggested by, among other clinical features, the presence of flat feet and history of hernia surgery.[11]
Use of this content is subject to our disclaimer