Investigations
1st investigations to order
haemoglobin (Hb)
Test
Hb will be normal in alpha-thalassaemia silent carrier and may be slightly low in alpha-thalassaemia trait.
The Hb level is variable in Hb H disease: approximately 70-110 g/L (7-11 g/dL) in deletional disease and 40-90 g/L (4-9 g/dL) in non-deletional disease.[16]
Result
normal to low
mean corpuscular volume (MCV)
Test
The MCV correlates with phenotypic and genotypic worsening of the disease. Patients with alpha-thalassaemia silent carrier have a normal to slightly low MCV, whereas those with deletional alpha-thalassaemia trait usually have an MCV of approximately 54 femtolitres (range 46-76 femtolitres).[16] Those with non-deletional Hb H disease will have an MCV of approximately 65 femtolitres (range 48.7 to 80.7 femtolitres).[16] Patients with Hb H/Constant Spring will have an MCV that is normal to mildly low, and those homozygous for Hb Constant Spring will often have a normal MCV.
Result
low
mean corpuscular haemoglobin (MCH)
Test
MCH will be normal to low (24-29 picograms/cell) in those with 1 alpha-thalassaemia silent carrier, and it will be low (<27 picograms/cell) in those with >1 alpha-globin deletion or in those with non-deletional mutations.
Mean MCH is approximately 17 picograms for deletional Hb H disease and 19 picograms for non-deletional Hb H disease.[16]
Result
low
red blood cell count
Test
Should be performed in all patients.
Result
increased; variable, corresponding to severity
peripheral smear
Test
Carefully review for findings consistent with alpha-thalassaemia, including microcytosis, hypochromia, increased polychromasia, target cells, and anisopoikilocytosis.[16]
Misshapen and even fragmented red cells may be found in patients with Hb H disease, and characteristic inclusion bodies may be seen on staining with a supravital dye such as brilliant cresyl blue.[16]
[Figure caption and citation for the preceding image starts]: Haemoglobin H diseaseFrom the collection of Elizabeth A. Price and Stanley L. Schrier, Stanford University [Citation ends].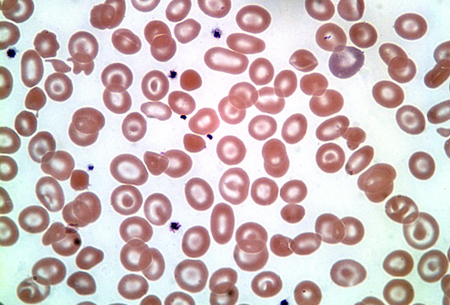
In homozygous Hb Constant Spring, the cells will be normal or slightly small in size, and basophilic stippling may be prominent.[6]
Result
abnormal shape and size of cells
reticulocyte percentage
Test
In Hb H disease, the reticulocyte percentage is elevated (2.5% to 4.0% for deletional Hb H; 5.5% to 6.5% for non-deletional Hb H) and may be further increased during acute infections or haemolytic crises.[16]
Result
increased
serum iron
Test
If microcytosis (MCV <78 femtolitres) or hypochromia (MCH <27 picograms) is present, iron status should be assessed to differentiate between anaemia due to thalassaemia and iron-deficiency anaemia.
Result
normal or elevated
serum ferritin
Test
If microcytosis (MCV <78 femtolitres) or hypochromia (MCH <27 picograms) is present, iron status should be assessed to differentiate between anaemia due to thalassaemia and iron-deficiency anaemia.
If serum ferritin levels suggest elevated iron status, liver iron overload should be assessed. Serum ferritin levels may underestimate liver iron concentration.[56]
Guidelines suggest MRI evaluation of liver iron if serum ferritin is >674.1 picomol/L (>300 nanograms/mL) in patients with Hb H disease.[16]
Result
normal or elevated
Investigations to consider
brilliant cresyl blue staining of red blood cells
Test
Numerous inclusion bodies are typically seen in Hb H disease.[16] Believed by some experts to be more reliable than Hb electrophoresis for diagnosis of Hb H disease.
May be reduced or absent in the presence of heterozygous beta-thalassaemia such as Hb S, Hb C, Hb E, or beta-thalassaemia.[46][57]
Result
demonstrates Hb H inclusions in peripheral blood red cells
Hb electrophoresis
Test
Hb H and Hb Bart can be detected as fast-moving haemoglobins. Will not pick up alpha-thalassaemia silent carrier or alpha-thalassaemia trait outside of the newborn period (Hb Barts), and will not differentiate deletional from non-deletional forms of Hb H (except for Hb Constant Spring). Patients with Hb H disease and concomitant heterozygous beta-haemoglobinopathies such as Hb S, Hb C, Hb E, or beta-thalassaemia have low or absent Hb H, which may confound the diagnosis of Hb H disease.
Result
presence of Hb H, Hb Bart, and concomitant haemoglobinopathies (Hb E, Hb S, Hb C, Hb D)
Hb fractionation by high-performance liquid chromatography (HPLC)
Test
Hb fractionation by HPLC provides fast separation and precise estimation of haemoglobin variants.
Will not pick up alpha-thalassaemia silent carrier or alpha-thalassaemia trait outside of the newborn period (Hb Barts), and will not differentiate deletional from non-deletional forms of Hb H (except for Hb Constant Spring). Patients with Hb H disease and concomitant heterozygous beta-haemoglobinopathies such as Hb S, Hb C, Hb E, or beta-thalassaemia have low or absent Hb H, which may confound the diagnosis of Hb H disease.
Result
presence of Hb H, Hb Bart, and concomitant haemoglobinopathies (Hb E, Hb S, Hb C, Hb D)
gap-polymerase chain reaction (gap-PCR)
Test
Seven of the most common alpha-thalassaemia deletions (-alpha(3.7), -alpha(4.2), --(FIL), --(THAI), --(MED), -(alpha)(20.5) , --(SEA)) can be diagnosed by gap-PCR.[16]
Result
detects specific deletions
multiplex ligation-dependent probe amplification
Test
Used to detect deletions and duplications in the alpha-globin gene cluster causing alpha-thalassaemia.[16]
Result
detects deletion alleles
direct sequencing/reverse dot blot
MRI (hepatic or cardiac)
Test
Liver iron overload can be assessed by R2 or R2* MRI.[16][55]
Guidelines suggest MRI evaluation of liver iron concentration if serum ferritin is >674.1 picomol/L (>300 nanograms/mL) in patients with Hb H disease.[16]
Cardiac iron loading is assessed by T2* cardiac MRI.[16] Cardiac iron loading is uncommon in non-transfused patients.
Result
liver or cardiac iron in patients with iron overload is demonstrated by difference in organ-to-muscle signal intensity
superconducting quantum interference devices (SQUID)
liver biopsy
Test
MRI is preferred to liver biopsy for assessment of iron overload where possible as it has better accuracy and fewer procedural risks. Liver biopsy may be used where assessment of histology is needed.[21]
Guidelines suggest evaluation of liver iron concentration if serum ferritin is >674.1 picomol/L (>300 nanograms/mL) in patients with Hb H disease.[16]
Result
liver iron ≥5 mg Fe/g dry weight on liver biopsy indicates need for iron chelation therapy
Use of this content is subject to our disclaimer