Epidemiology
Data on incidence and outcome parameters such as in-hospital mortality are sparse. Two studies in the US showed an incidence of upper gastrointestinal haemorrhage of between 60 and 78 per 100,000 population in 2009.[8][9] In one German study based on standardised hospital discharge data provided by the German Federal Statistical Office between 2010 and 2019, an average of approximately 6000 patients per year had MWT, with an overall annual hospitalisation incidence of 7.5/100,000 persons and an in hospital mortality rate of 2.7%.[10]
MWT represents approximately 5% to 7% of patients with upper GI bleeding.[11] It is less common in children, representing about 0.3% of upper GI bleeds.[12] MWT is more common in men than in women in a ratio of 3:1.[13] In women of childbearing age, the most common cause is hyperemesis gravidarum.[14] MWT has no racial predilection. The age of presentation may vary but is most common in people aged between 30 and 50 years.[12] Recurrent bleeding after an episode of MWT has been reported to occur in around 10% of patients.[15][16]
Risk factors
Conditions that may induce vomiting include food poisoning, gastroenteritis, or any gastrointestinal condition resulting in obstruction; hepatitis, gallstones, and cholecystitis; hyperemesis gravidarum; urinary tract infection, renal failure, and ureteropelvic obstruction; brain tumours, hydrocephalus, congenital disease, trauma, meningitis, intracranial hypertension, migraine headaches, and seizures; anorexia nervosa, bulimia, and cyclic vomiting syndrome; toxins, chemotherapy agents, and post-anaesthesia or post-surgery.[14][19][20][21][22][23][24]
May be associated with whooping cough, bronchitis, bronchiectasis, emphysema, COPD, or lung cancer.[25]
Mucosal tear or laceration during a routine endoscopy is a rare event (0.0001% to 0.4% of people undergoing endoscopy).[26][27] However, it is considered to be the most common cause of iatrogenic tear or laceration.
Other procedures involving instrumentation that may be associated with oesophageal tear or laceration include naso- or orogastric tube placement, endoscope band ligation, endoscopic retrograde cholangiopancreatography, and endoscopic ultrasound.[28][Figure caption and citation for the preceding image starts]: Bleeding Mallory Weiss Tear viewed on retroflexionFrom the personal collection of Douglas Adler; used with permission [Citation ends].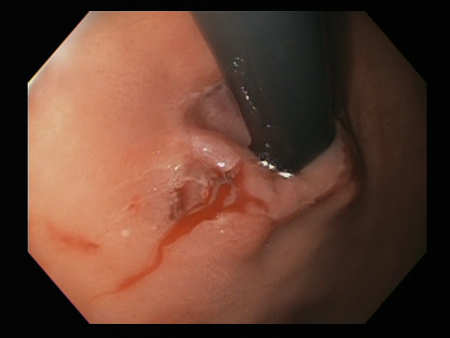
History of significant alcohol use and vomiting is common in patients who present with MWT. Alcohol use is present in 30% to 60% of patients.[1]
More common in men than in women in a ratio of 3:1.[13]
A sudden increase of intraluminal pressure against a closed glottis has been suggested as the main mechanism for development of MWT, although the pathogenesis is uncertain.[32] Blunt abdominal trauma is one of the mechanisms by which intraluminal pressure can increase.
Exact pathogenesis is uncertain, although compression of the oesophagus between the sternum and the vertebrae is probably the most likely explanation.[33]
Use of this content is subject to our disclaimer